

A comparative analysis on characteristics and mortalities of four key transmission populations on antiretroviral therapy: a retrospective cohort study in Northwest China
- PMID: 35346084
- PMCID: PMC8962555
- DOI: 10.1186/s12879-022-07281-x
A comparative analysis on characteristics and mortalities of four key transmission populations on antiretroviral therapy: a retrospective cohort study in Northwest China
Abstract
Background: This study explored disparities in characteristics and mortalities among four major transmission groups on antiretroviral therapy in northwest China as well as the survival impact of each transmission route.
Methods: We first examined disparities in demographics and clinical characteristics of the four transmission populations. Kaplan Meier analysis was subsequently conducted to compare survival rates among all groups. At last, Cox proportional hazards regression model was employed to analyze the survival impact of a transmission route among seven main categories of survival factors associated with all-cause mortalities.
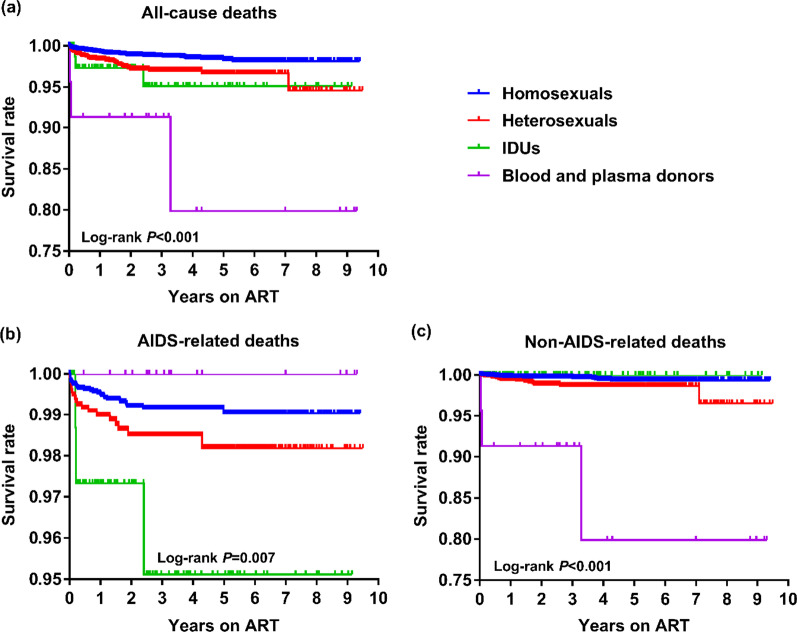
Results: Survival analysis showed significant differences in all-cause, AIDS- and non-AIDS-related deaths among four HIV populations (all P < 0.05). Using homosexuals as the reference, Cox proportional hazards model further revealed that the risk of all-cause death for blood and plasma donors was significantly higher than that of the reference (aHR: 5.21, 95%CI: 1.54-17.67); the risk of non-AIDS-related death for heterosexuals (aHR: 2.07, 95%CI: 1.01-4.20) and that for blood and plasma donors (aHR: 19.81, 95%CI: 5.62-69.89) were both significantly higher than that of the reference.
Conclusions: Significant disparities were found in characteristics and mortalities among the four transmission groups where mortality disparities were mainly due to non-AIDS-related death. Suggestions are provided for each group to improve their survivorship.
Keywords: Antiretroviral therapy; Cohort study; HIV/AIDS; Homosexuals; Transmission category.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
[Survival analysis on Former Plasma Donors living with HIV/AIDS after initiation of antiretroviral therapy in Henan province, 2002-2017].Zhonghua Liu Xing Bing Xue Za Zhi. 2019 Jun 10;40(6):638-642. doi: 10.3760/cma.j.issn.0254-6450.2019.06.007. Zhonghua Liu Xing Bing Xue Za Zhi. 2019. PMID: 31238611 Chinese.
-
[Survival time of HIV/AIDS cases and influencing factors in Gansu province, 1997-2018].Zhonghua Liu Xing Bing Xue Za Zhi. 2019 Nov 10;40(11):1398-1402. doi: 10.3760/cma.j.issn.0254-6450.2019.11.011. Zhonghua Liu Xing Bing Xue Za Zhi. 2019. PMID: 31838811 Chinese.
-
Effect of AIDS-defining events at initiation of antiretroviral therapy on long-term mortality of HIV/AIDS patients in Southwestern China: a retrospective cohort study.AIDS Res Ther. 2020 Jul 17;17(1):44. doi: 10.1186/s12981-020-00300-4. AIDS Res Ther. 2020. PMID: 32680536 Free PMC article.
-
Effect of antiretroviral therapy initiation time and baseline CD4+ cell counts on AIDS-related mortality among former plasma donors in China: a 21-year retrospective cohort study.Glob Health Action. 2021 Jan 1;14(1):1963527. doi: 10.1080/16549716.2021.1963527. Glob Health Action. 2021. PMID: 34592916 Free PMC article.
-
[Survival analysis of AIDS patients in Liangshan prefecture, Sichuan province from 1995 to 2012].Zhonghua Yu Fang Yi Xue Za Zhi. 2014 Aug;48(8):678-83. Zhonghua Yu Fang Yi Xue Za Zhi. 2014. PMID: 25388462 Chinese.
Cited by
-
Survival analysis of PLWH on antiretroviral therapy in Henan Province from 2004 to 2024.Sci Rep. 2025 Jul 1;15(1):21322. doi: 10.1038/s41598-025-05821-4. Sci Rep. 2025. PMID: 40593096 Free PMC article.
References
-
- Boulle A, Schomaker M, May MT, Hogg RS, Shepherd BE, Monge S, Keiser O, Lampe FC, Giddy J, Ndirangu J, et al. Mortality in patients with HIV-1 infection starting antiretroviral therapy in South Africa, Europe, or North America: a collaborative analysis of prospective studies. PLoS Med. 2014;11(9):e1001718. doi: 10.1371/journal.pmed.1001718. - DOI - PMC - PubMed
-
- Mocroft A, Vella S, Benfield TL, Chiesi A, Miller V, Gargalianos P, d'Arminio Monforte A, Yust I, Bruun JN, Phillips AN, et al. Changing patterns of mortality across Europe in patients infected with HIV-1. EuroSIDA Study Group. Lancet (London, England). 1998;352(9142):1725–1730. doi: 10.1016/S0140-6736(98)03201-2. - DOI - PubMed
-
- Zhao Y, Wu Z, McGoogan JM, Shi CX, Li A, Dou Z, Ma Y, Qin Q, Brookmeyer R, Detels R, et al. Immediate antiretroviral therapy decreases mortality among patients with high CD4 counts in China: a nationwide, retrospective cohort study. Clin Infect Dis. 2018;66(5):727–734. doi: 10.1093/cid/cix878. - DOI - PMC - PubMed
-
- UNAIDS. Global HIV & AIDS statistics—2020 fact sheet. 2020. https://www.unaids.org/en/resources/fact-sheet. Accessed 2 Sep 2021.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
