

Recurrence and prognosis in intrahepatic cholangiocarcinoma patients with different etiology after radical resection: a multi-institutional study
- PMID: 35346122
- PMCID: PMC8962079
- DOI: 10.1186/s12885-022-09448-w
Recurrence and prognosis in intrahepatic cholangiocarcinoma patients with different etiology after radical resection: a multi-institutional study
Abstract
Objective: We aimed to evaluate the prognosis and adjuvant chemotherapy (ACT) in intrahepatic cholangiocarcinoma (ICC) patients with different etiology after radical resection.
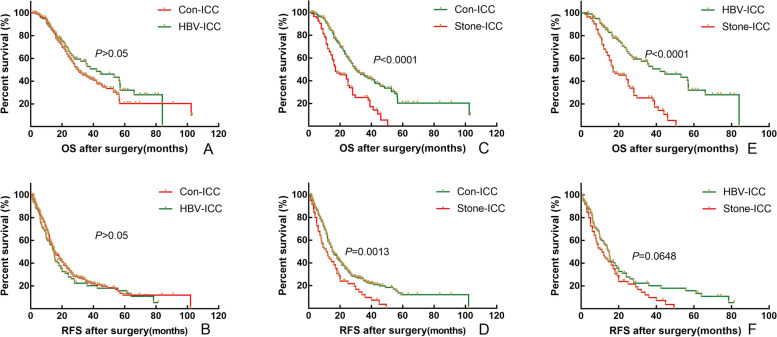
Methods: A total of 448 patients with ICC who underwent radical resection between 2010 and 2018 at ten Chinese tertiary hospitals were analyzed in the study. These patients were divided into conventional ICC (Con-ICC, n = 261, 58.2%), hepatitis B virus ICC (HBV-ICC, n = 102, 22.8%) and hepatolithiasis (Stone-ICC, n = 85,19.0%) subtypes according to different etiology. Propensity score matching (PSM) was conducted to mitigate the baseline differences between Con-ICC and HBV-ICC, Con-ICC and Stone-ICC, HBV-ICC and Stone-ICC subtypes.
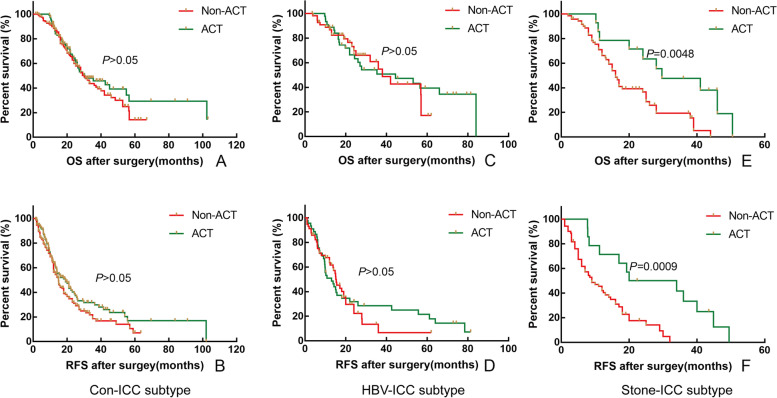
Results: Univariate and multivariate analysis showed that different etiology was a prognostic factor for overall survival and relapse-free survival, and different etiology was an independent risk factor for overall survival in ICC patients, respectively (P < 0.05). In addition, there was a statistical difference for overall survival in early recurrence patients among the three etiological subtypes (P < 0.05). After PSM, the overall survival of patients with Stone-ICC was worse than those of Con-ICC and HBV-ICC subtypes (P < 0.05), while the relapse-free survival of patients with Stone-ICC was equivalent to patients with Con-ICC and HBV-ICC (P > 0.05). In Stone-ICC patients, the median overall survival was 16.0 months and 29.7 months, and the median relapse-free survival was 9.0 months and 20.0 months for non-ACT and ACT patients, respectively (P < 0.05).
Conclusion: The prognosis of Stone-ICC patients was significantly worse than those of Con-ICC and HBV-ICC patients. Interestingly, postoperative adjuvant chemotherapy can improve the prognosis of Stone-ICC patients effectively.
Keywords: Hepatitis B virus; Hepatolithiasis; Intrahepatic cholangiocarcinoma; Prognosis; Recurrence.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
Publication types
MeSH terms
Grants and funding
- No. 62076194, No. 81772521/National Natural Science Foundation of China
- No. 62076194, No. 81772521/National Natural Science Foundation of China
- DLY201807/Multicenter Clinical Research Project of Shanghai Jiaotong University, School of Medicine
- 17CSK06/Clinical Training Program of Shanghai Xinhua Hospital Affiliated to Shanghai Jiaotong University, School of Medicine
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
