

Antimicrobial stewardship in high-risk febrile neutropenia patients
- PMID: 35346373
- PMCID: PMC8961889
- DOI: 10.1186/s13756-022-01084-0
Antimicrobial stewardship in high-risk febrile neutropenia patients
Abstract
Background: The 2011 4th European Conference on Infections in Leukemia (ECIL4) guidelines recommend antibiotics de-escalation/discontinuation in selected febrile neutropenia (FN) patients. We aimed to assess the impact of an antimicrobial stewardship (AMS) program based on these guidelines on antibiotics use and clinical outcomes in high-risk FN patients.
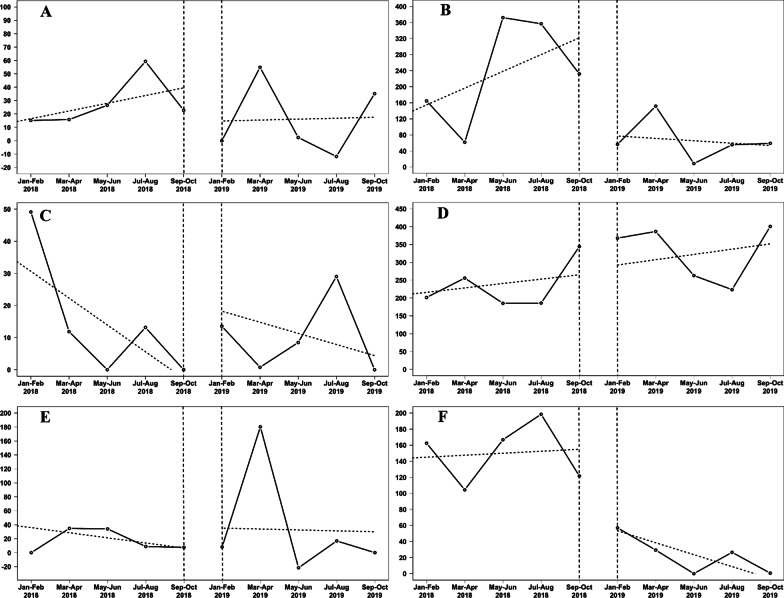
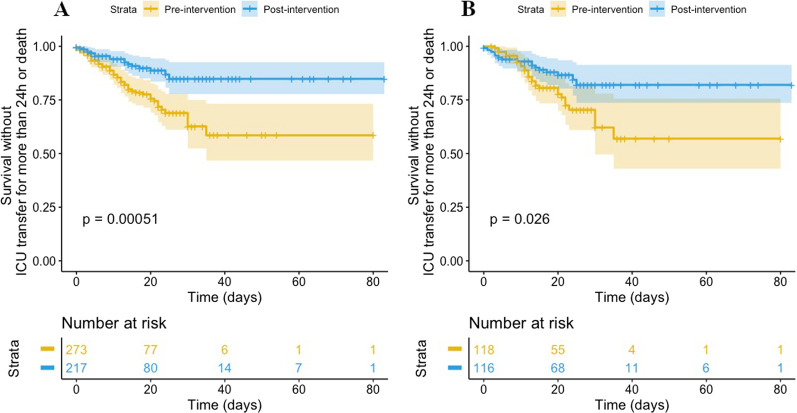
Methods: We conducted an observational study in the hematology department of Cochin University Hospital in Paris, France. An ECIL4-based antibiotics de-escalation and discontinuation strategy was implemented jointly by the hematologists and the AMS team. The pre-intervention (January-October 2018) and post-intervention (January-October 2019) periods were compared. We retrospectively collected clinical and microbiological data. We compiled antibiotics consumptions via hospital pharmacy data and standardized them by calculating defined daily doses per 1000 patient-days. We analyzed the two-monthly antibiotic consumption using an interrupted time series method and built a composite endpoint for clinical outcomes based on transfer to the intensive care unit (ICU) and/or hospital death.
Results: Overall, 273 hospital stays (164 patients) in the pre-intervention and 217 (148 patients) in the post-intervention periods were analyzed. Patients were mainly hospitalized for intensive chemotherapy for acute leukemia or autologous stem-cell transplant for myeloma. Patients were slightly younger in the pre-intervention compared to the post-intervention period (median age 60.4 vs 65.2 years, p = 0.049), but otherwise comparable. After implementation of the AMS program, glycopeptide and carbapenem use decreased by 85% (p = 0.03) and 72% (p = 0.04), respectively. After adjustment on confounders, the risk of transfer to the ICU/death decreased significantly after implementation of the AMS program (post-intervention period: odds-ratio = 0.29, 95% Confidence Interval: 0.15-0.53, p < 0.001).
Conclusion: Implementation of a multidisciplinary AMS program for high-risk neutropenic patients was associated with lower carbapenem and glycopeptide use and improved clinical outcomes.
Keywords: Antibiotic consumption; Antimicrobial stewardship; High-risk febrile neutropenia; Prognosis.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Averbuch D, Orasch C, Cordonnier C, Livermore DM, Mikulska M, Viscoli C, et al. European guidelines for empirical antibacterial therapy for febrile neutropenic patients in the era of growing resistance: summary of the 2011 4th European Conference on Infections in Leukemia. Haematologica. 2013;98(12):1826–35. doi: 10.3324/haematol.2013.091025. - DOI - PMC - PubMed
-
- Aguilar-Guisado M, Espigado I, Martín-Peña A, Gudiol C, Royo-Cebrecos C, Falantes J, et al. Optimisation of empirical antimicrobial therapy in patients with haematological malignancies and febrile neutropenia (How Long study): an open-label, randomised, controlled phase 4 trial. Lancet Haematol. 2017;4(12):e573–e583. doi: 10.1016/S2352-3026(17)30211-9. - DOI - PubMed
-
- la Martire G, Robin C, Oubaya N, Lepeule R, Beckerich F, Leclerc M, et al. De-escalation and discontinuation strategies in high-risk neutropenic patients: an interrupted time series analyses of antimicrobial consumption and impact on outcome. Eur J Clin Microbiol Infect Dis. 2018;37(10):1931–1940. doi: 10.1007/s10096-018-3328-1. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
