

Cumulative burden of psychiatric disorders and self-harm across 26 adult cancers
- PMID: 35347280
- PMCID: PMC9018408
- DOI: 10.1038/s41591-022-01740-3
Cumulative burden of psychiatric disorders and self-harm across 26 adult cancers
Abstract
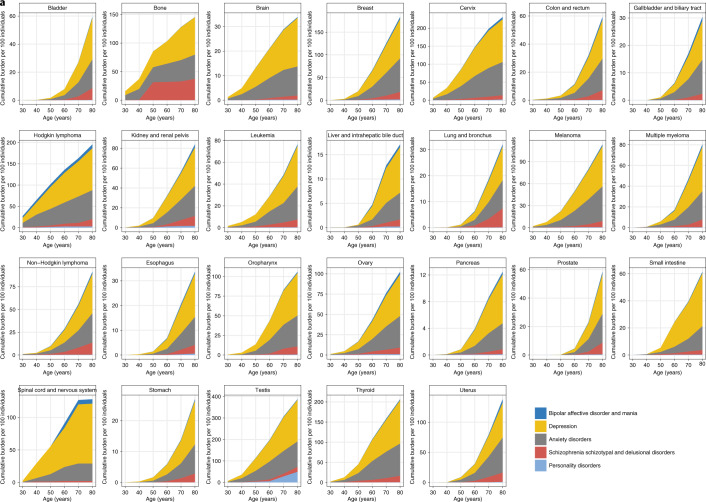
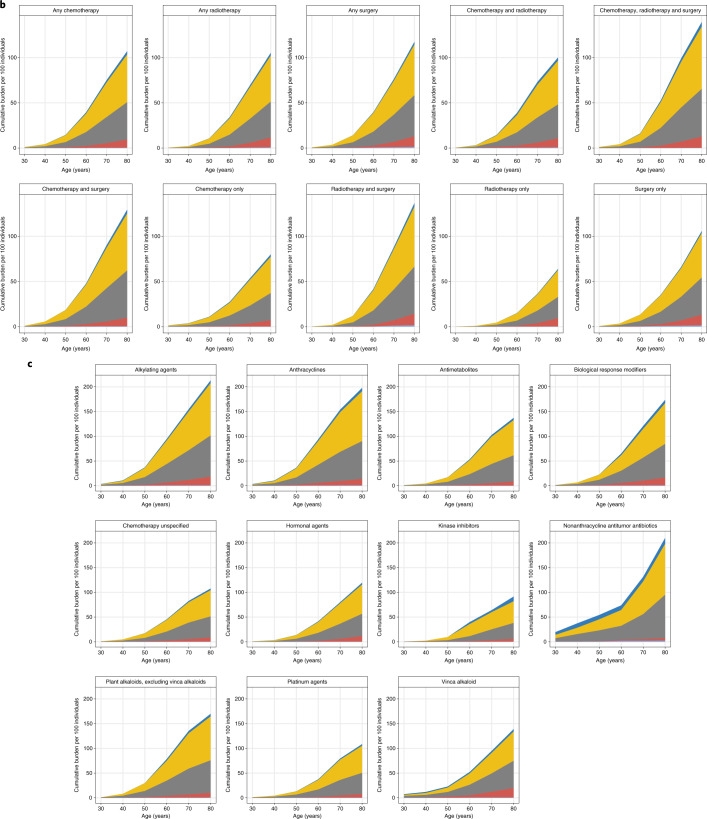
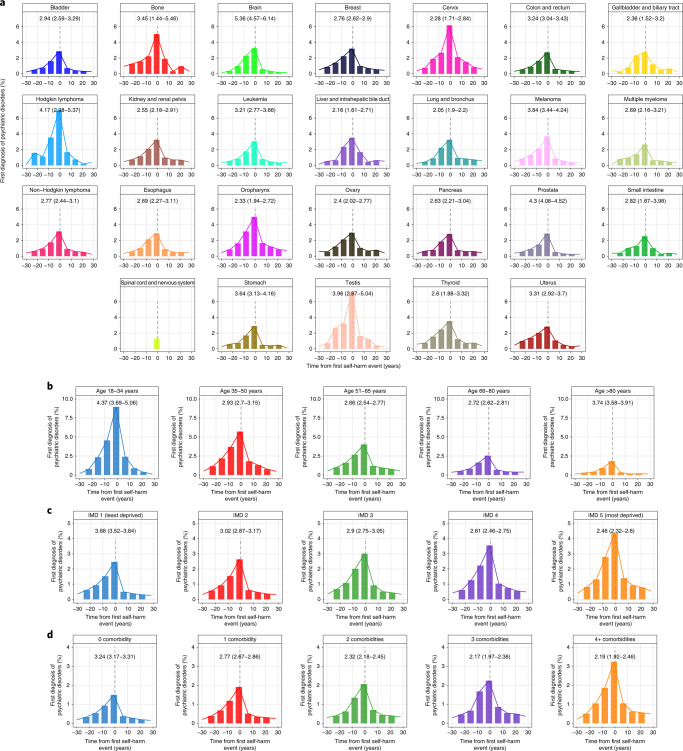
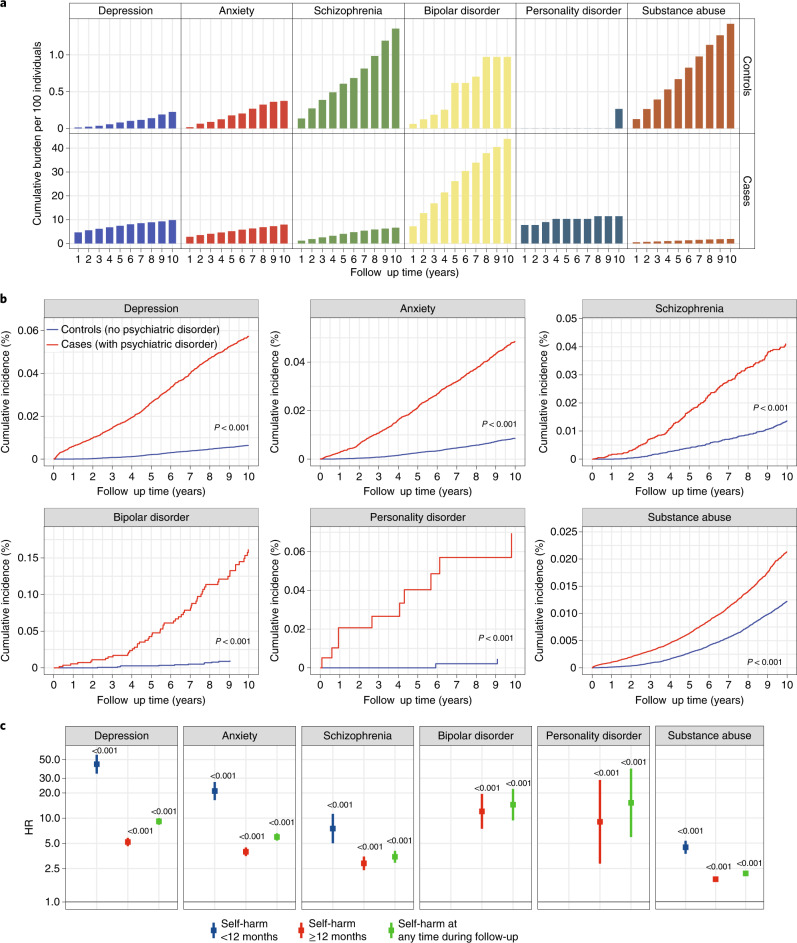
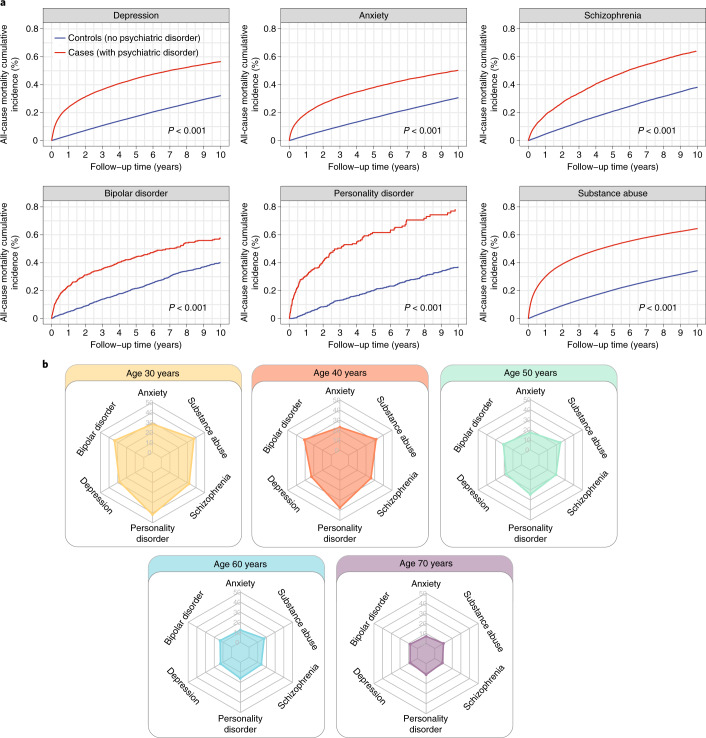
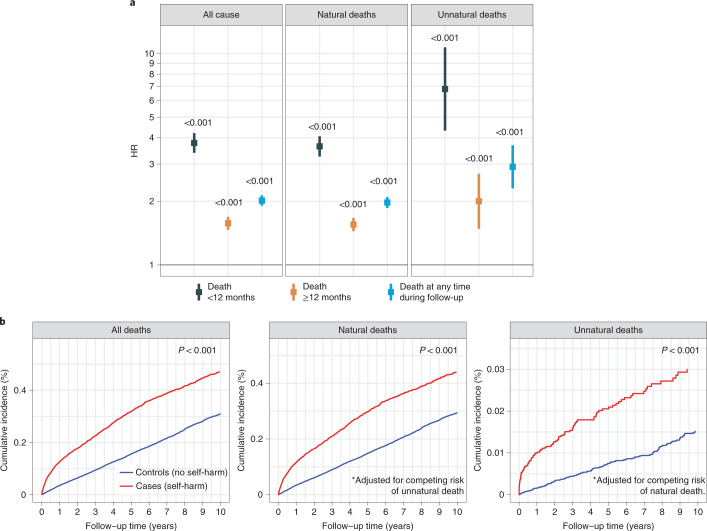
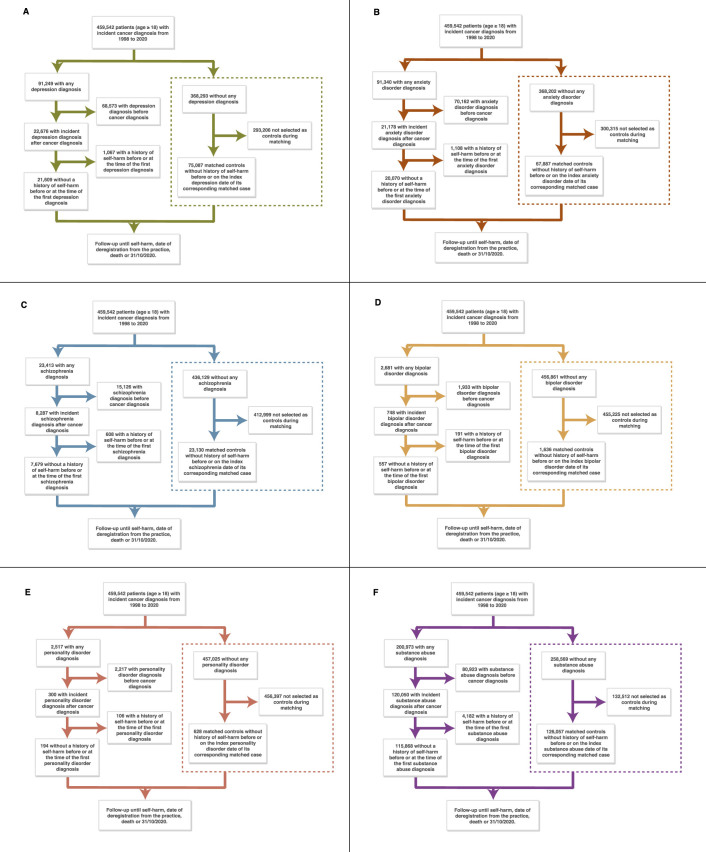
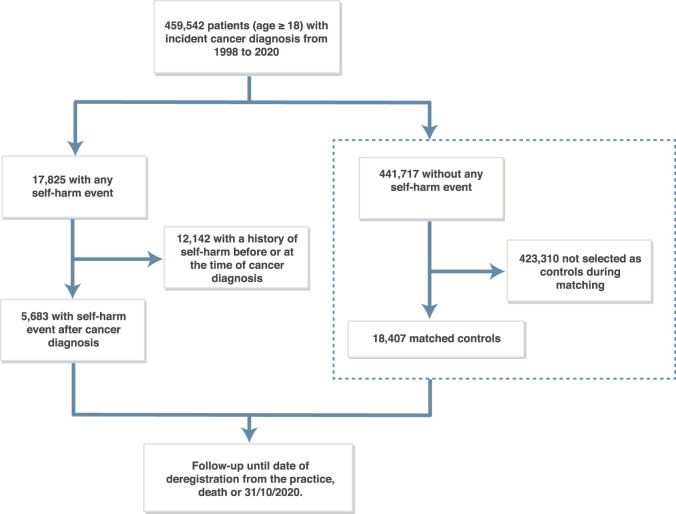
Cancer is a life-altering event causing considerable psychological distress. However, information on the total burden of psychiatric disorders across all common adult cancers and therapy exposures has remained scarce. Here, we estimated the risk of self-harm after incident psychiatric disorder diagnosis in patients with cancer and the risk of unnatural deaths after self-harm in 459,542 individuals. Depression was the most common psychiatric disorder in patients with cancer. Patients who received chemotherapy, radiotherapy and surgery had the highest cumulative burden of psychiatric disorders. Patients treated with alkylating agent chemotherapeutics had the highest burden of psychiatric disorders, whereas those treated with kinase inhibitors had the lowest burden. All mental illnesses were associated with an increased risk of subsequent self-harm, where the highest risk was observed within 12 months of the mental illness diagnosis. Patients who harmed themselves were 6.8 times more likely to die of unnatural causes of death compared with controls within 12 months of self-harm (hazard ratio (HR), 6.8; 95% confidence interval (CI), 4.3-10.7). The risk of unnatural death after 12 months was markedly lower (HR, 2.0; 95% CI, 1.5-2.7). We provide an extensive knowledge base to help inform collaborative cancer-psychiatric care initiatives by prioritizing patients who are most at risk.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Comment in
-
Shining a light on the psychological burden of cancer.Nat Med. 2022 Apr;28(4):637-638. doi: 10.1038/s41591-022-01763-w. Nat Med. 2022. PMID: 35347283 No abstract available.
-
Suicide prevention in cancer: earlier is better.Trends Mol Med. 2022 Jun;28(6):437-438. doi: 10.1016/j.molmed.2022.04.009. Epub 2022 May 7. Trends Mol Med. 2022. PMID: 35537988
-
Patients with cancer have a higher suicide risk: Two new reports conclude that people with cancer are at higher risk for suicide and self-harm: Two new reports conclude that people with cancer are at higher risk for suicide and self-harm.Cancer. 2022 Sep 15;128(18):3275-3276. doi: 10.1002/cncr.34430. Cancer. 2022. PMID: 36018006 No abstract available.
References
-
- Pitman A, Suleman S, Hyde N, Hodgkiss A. Depression and anxiety in patients with cancer. BMJ. 2018;361:1–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
