

Molecular consequences of SARS-CoV-2 liver tropism
- PMID: 35347318
- PMCID: PMC8964418
- DOI: 10.1038/s42255-022-00552-6
Molecular consequences of SARS-CoV-2 liver tropism
Abstract
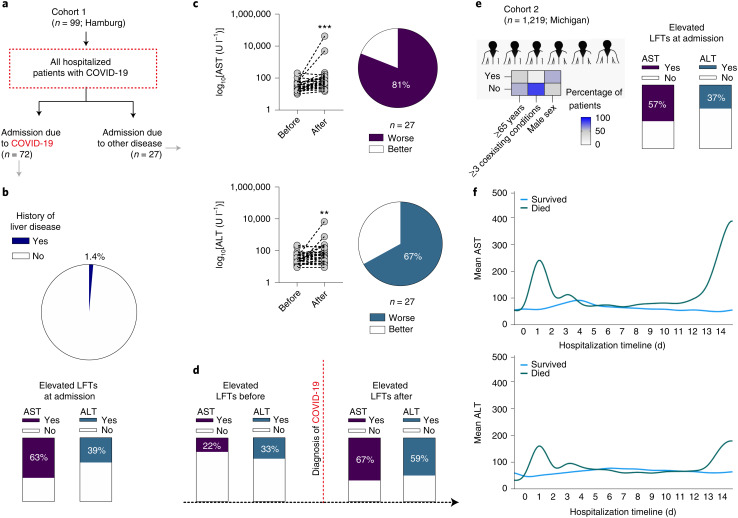
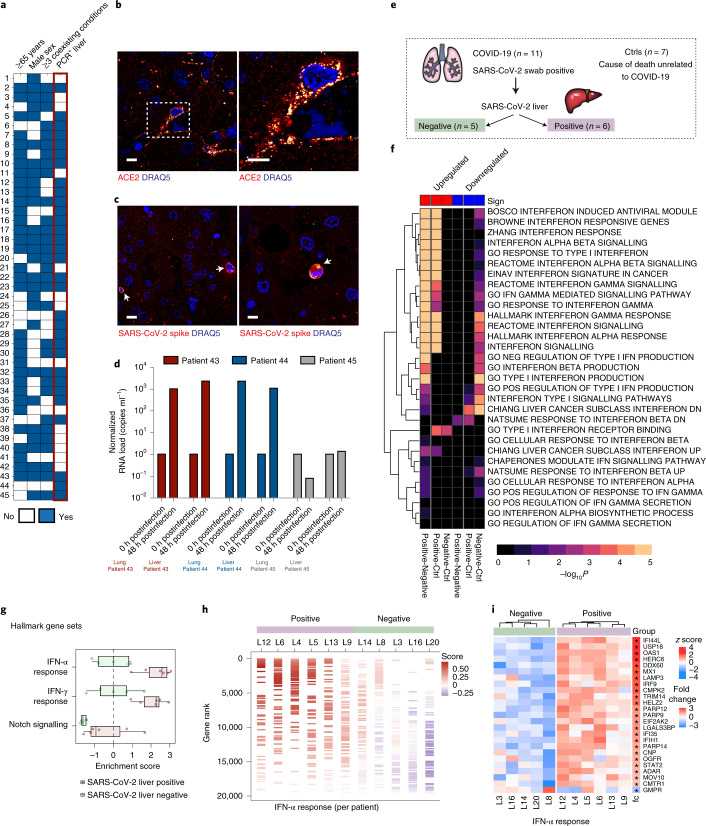
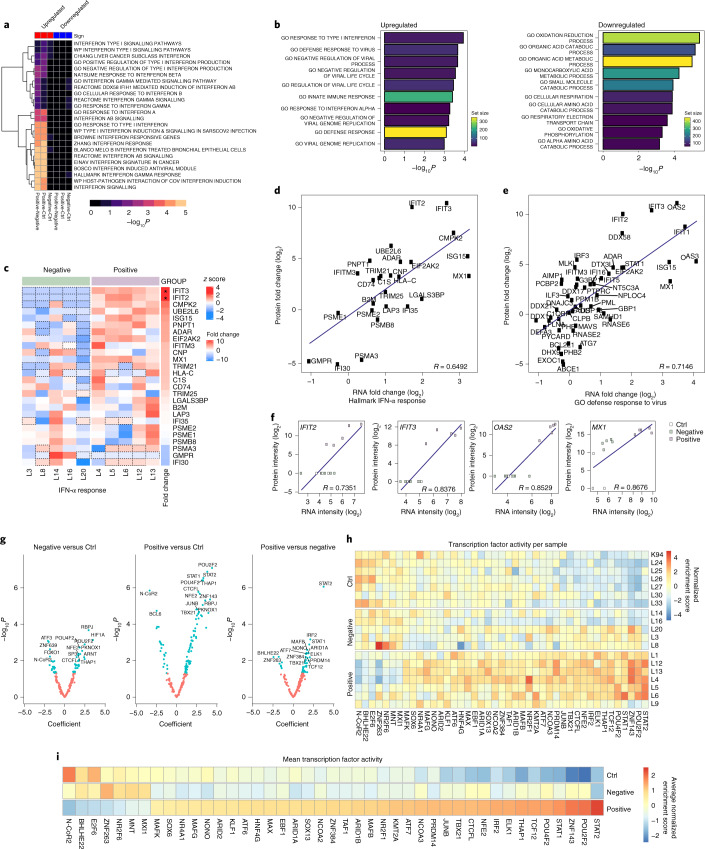
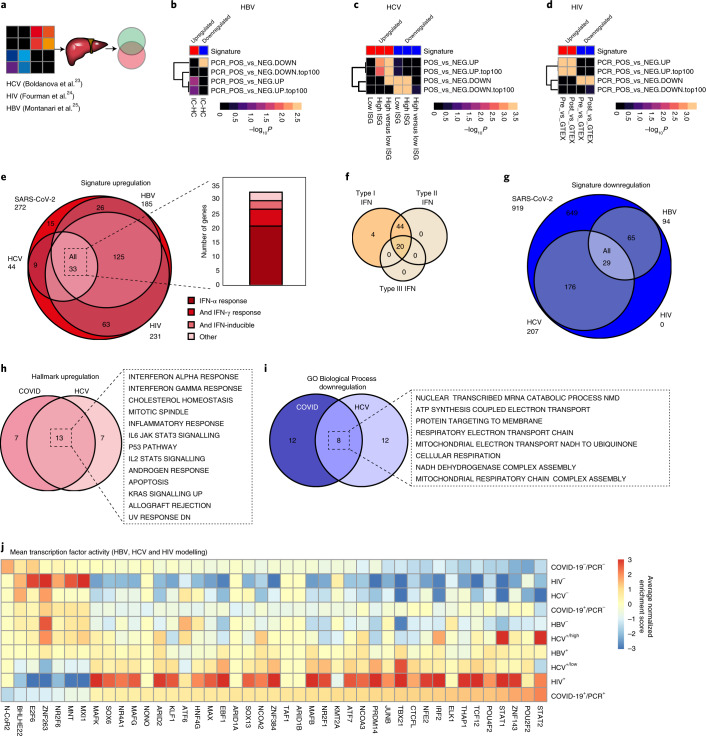
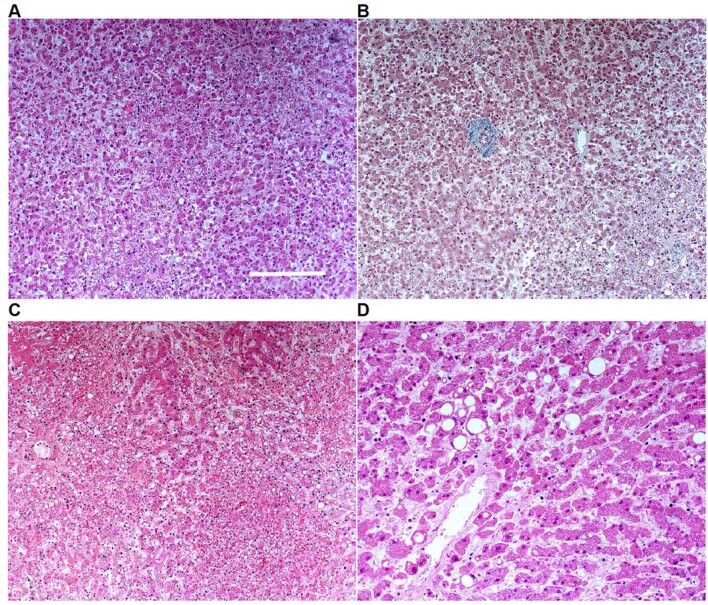
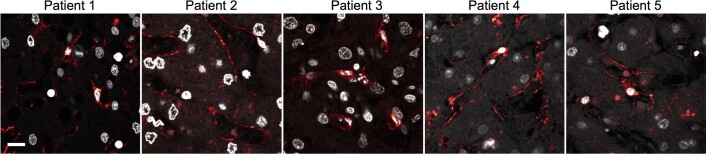
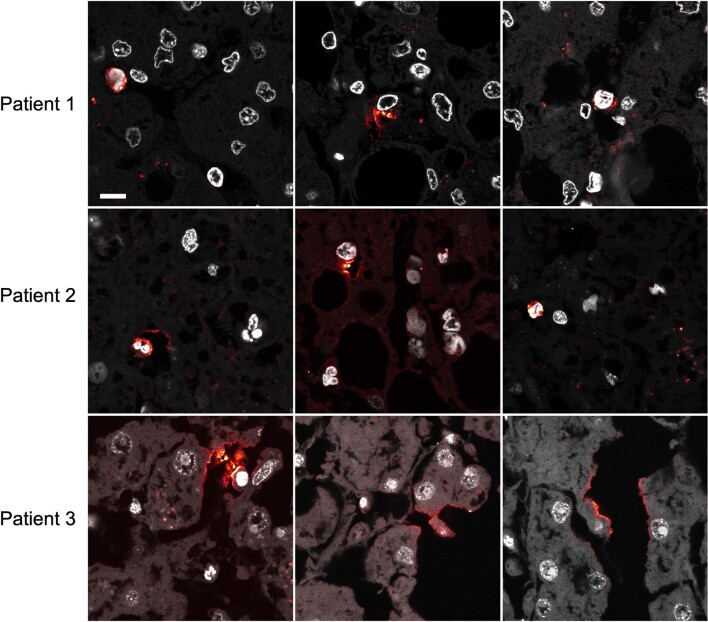
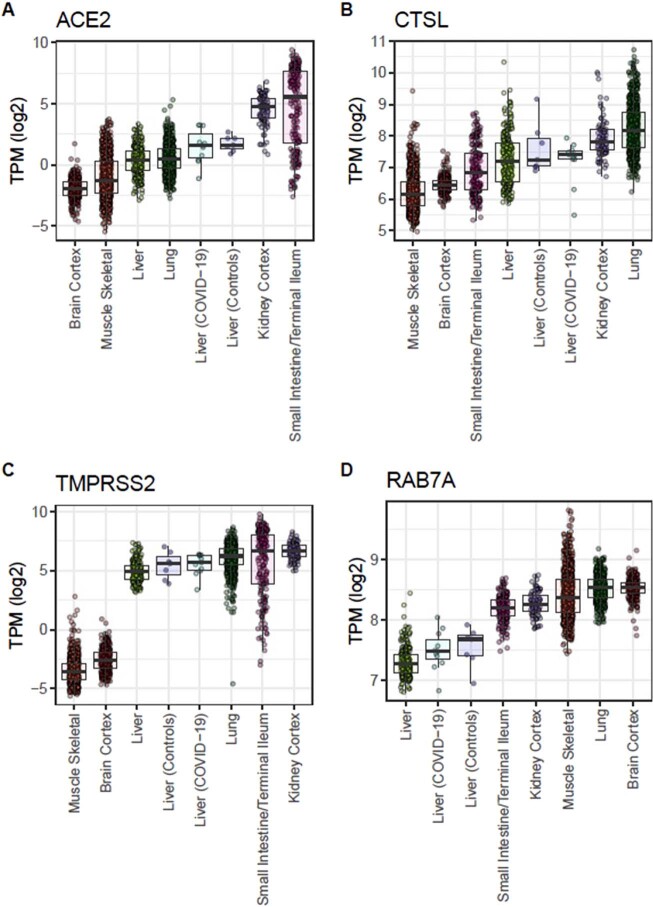
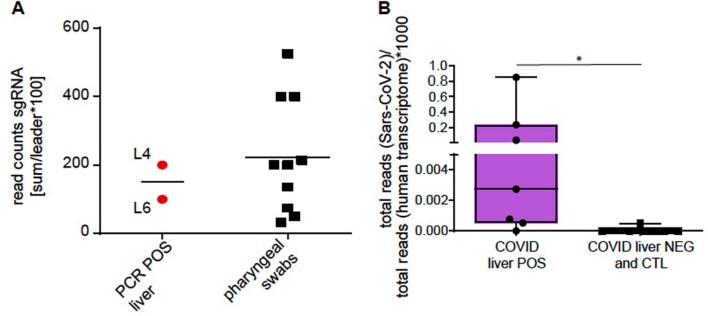
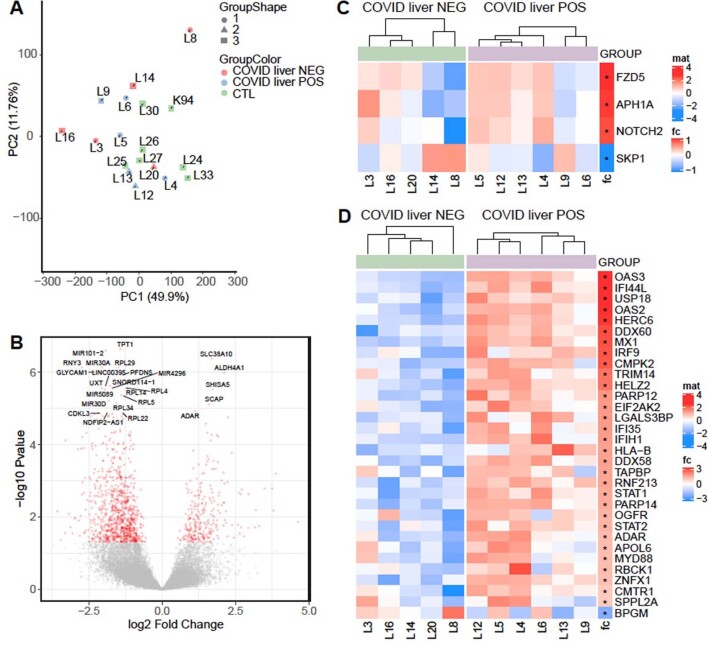
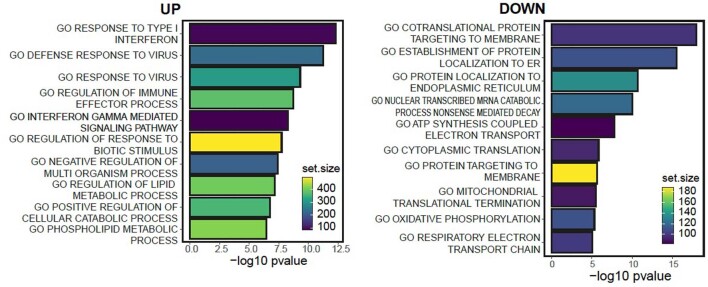
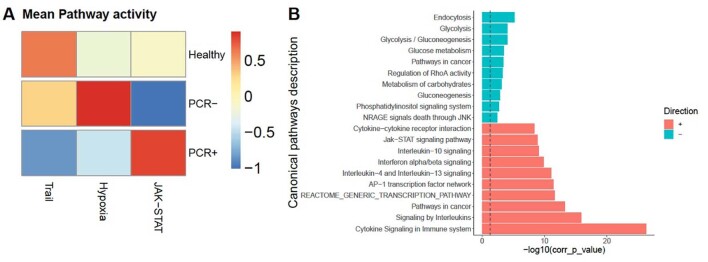
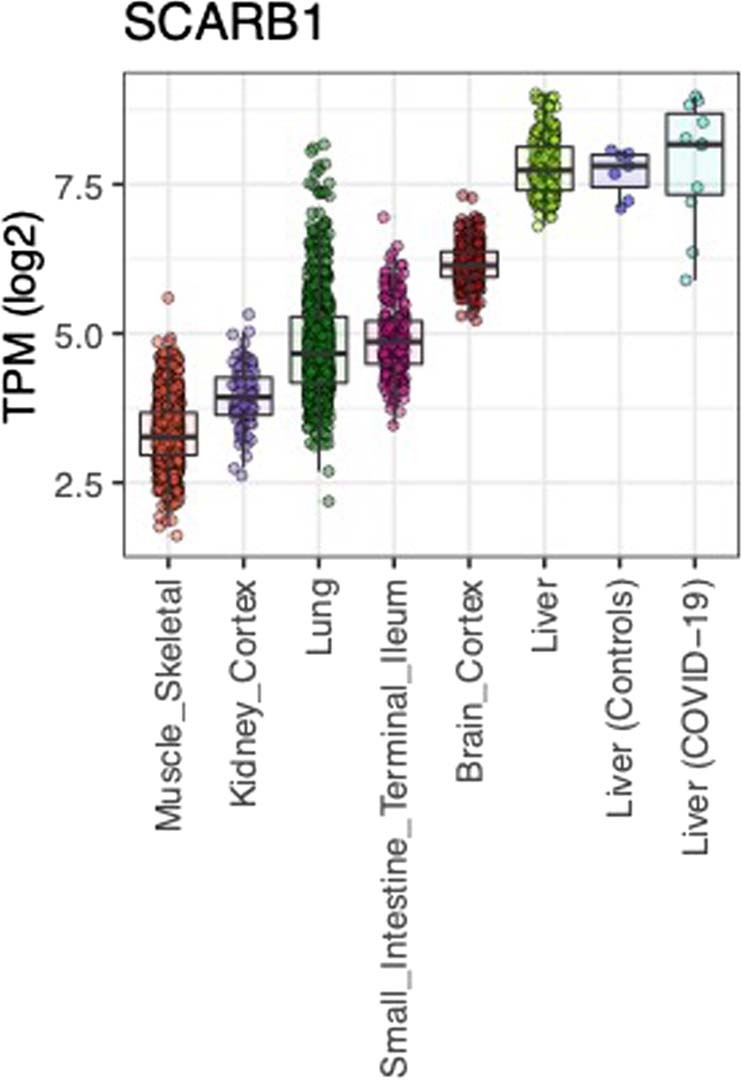
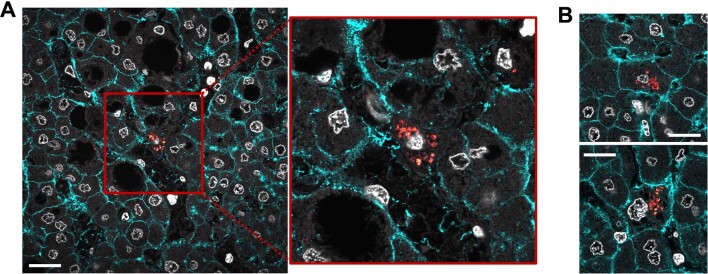
Extrapulmonary manifestations of COVID-19 have gained attention due to their links to clinical outcomes and their potential long-term sequelae1. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) displays tropism towards several organs, including the heart and kidney. Whether it also directly affects the liver has been debated2,3. Here we provide clinical, histopathological, molecular and bioinformatic evidence for the hepatic tropism of SARS-CoV-2. We find that liver injury, indicated by a high frequency of abnormal liver function tests, is a common clinical feature of COVID-19 in two independent cohorts of patients with COVID-19 requiring hospitalization. Using autopsy samples obtained from a third patient cohort, we provide multiple levels of evidence for SARS-CoV-2 liver tropism, including viral RNA detection in 69% of autopsy liver specimens, and successful isolation of infectious SARS-CoV-2 from liver tissue postmortem. Furthermore, we identify transcription-, proteomic- and transcription factor-based activity profiles in hepatic autopsy samples, revealing similarities to the signatures associated with multiple other viral infections of the human liver. Together, we provide a comprehensive multimodal analysis of SARS-CoV-2 liver tropism, which increases our understanding of the molecular consequences of severe COVID-19 and could be useful for the identification of organ-specific pharmacological targets.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Comment in
-
Multi-omic Characterization of COVID Hepatitis.Gastroenterology. 2022 Jul;163(1):335. doi: 10.1053/j.gastro.2022.05.004. Epub 2022 May 2. Gastroenterology. 2022. PMID: 35513009 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Grants and funding
- U01 DK119083/DK/NIDDK NIH HHS/United States
- CRC/841/Deutsche Forschungsgemeinschaft (German Research Foundation)
- SC 314/1-1/Deutsche Forschungsgemeinschaft (German Research Foundation)
- MIRACUM Consortia FKZ 01ZZ1801B/Bundesministerium für Bildung und Forschung (Federal Ministry of Education and Research)
- HU 1016/8-2/Deutsche Forschungsgemeinschaft (German Research Foundation)
- 1R01DK12801201A1/DK/NIDDK NIH HHS/United States
- R01 HL153384/HL/NHLBI NIH HHS/United States
- STOP-FSGS- 01GM1901C/Bundesministerium für Bildung und Forschung (Federal Ministry of Education and Research)
- CRC1479/Deutsche Forschungsgemeinschaft (German Research Foundation)
- eMed Consortia Fibromap/Bundesministerium für Bildung und Forschung (Federal Ministry of Education and Research)
- TRR167 (Z1)/Deutsche Forschungsgemeinschaft (German Research Foundation)
- HU 1016/11-1/Deutsche Forschungsgemeinschaft (German Research Foundation)
- CRC/1453 Project ID 431984000 - S1/Deutsche Forschungsgemeinschaft (German Research Foundation)
- HU 1016/12-1/Deutsche Forschungsgemeinschaft (German Research Foundation)
- CRC/1192/Deutsche Forschungsgemeinschaft (German Research Foundation)
- TTU 01.921/Deutsches Zentrum für Infektionsforschung (German Center for Infection Research)
- TTU 01.901/Deutsches Zentrum für Infektionsforschung (German Center for Infection Research)
- CRC/1160/Deutsche Forschungsgemeinschaft (German Research Foundation)
- U01-DK119083-03S1/DK/NIDDK NIH HHS/United States
- DEFEAT PANDEMIcs/Bundesministerium für Bildung und Forschung (Federal Ministry of Education and Research)
- CRC/850/Deutsche Forschungsgemeinschaft (German Research Foundation)
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
