

Mathematical modelling of oxygenation under veno-venous ECMO configuration using either a femoral or a bicaval drainage
- PMID: 35347456
- PMCID: PMC8960524
- DOI: 10.1186/s40635-022-00434-x
Mathematical modelling of oxygenation under veno-venous ECMO configuration using either a femoral or a bicaval drainage
Abstract
Background: The bicaval drainage under veno-venous extracorporeal membrane oxygenation (VV ECMO) was compared in present experimental study to the inferior caval drainage in terms of systemic oxygenation.
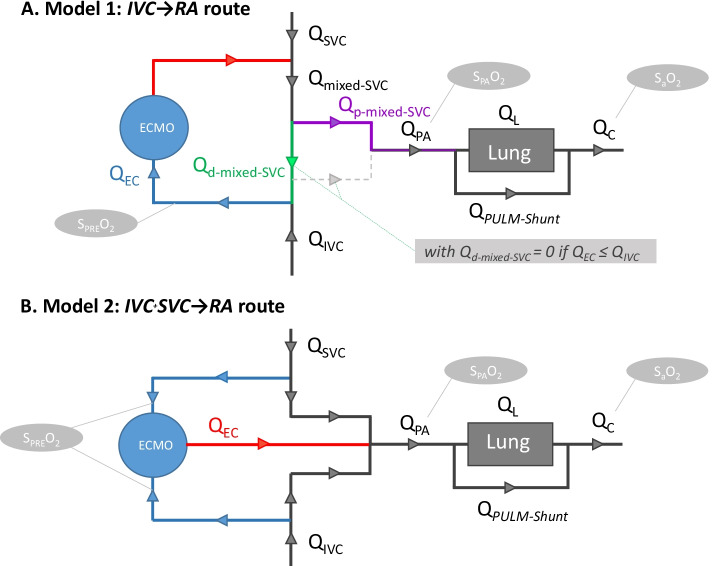
Method: Two mathematical models were built to simulate the inferior vena cava-to-right atrium (IVC → RA) route and the bicaval drainage-to-right atrium return (IVC + SVC → RA) route using the following parameters: cardiac output (QC), IVC flow/QC ratio, venous oxygen saturation, extracorporeal pump flow (QEC), and pulmonary shunt (PULM-Shunt) to obtain pulmonary artery oxygen saturation (SPAO2) and systemic blood oxygen saturation (SaO2).
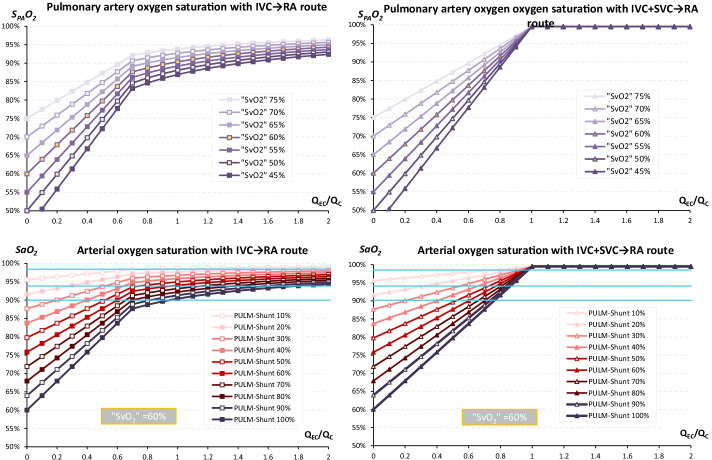
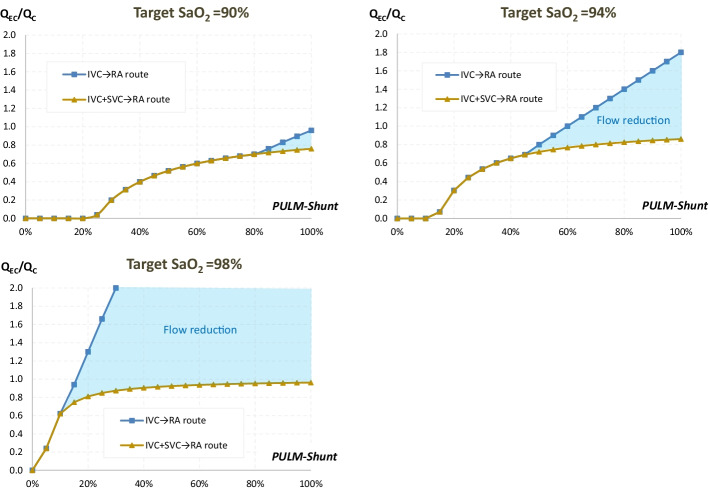
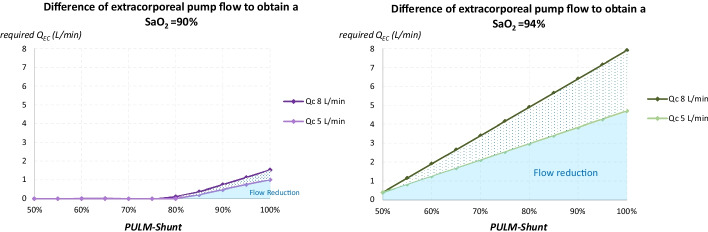
Results: With the IVC → RA route, SPAO2 and SaO2 increased linearly with QEC/QC until the threshold of the IVC flow/QC ratio, beyond which the increase in SPAO2 reached a plateau. With the IVC + SVC → RA route, SPAO2 and SaO2 increased linearly with QEC/QC until 100% with QEC/QC = 1. The difference in required QEC/QC between the two routes was all the higher as SaO2 target or PULM-Shunt were high, and occurred all the earlier as PULM-Shunt were high. The required QEC between the two routes could differ from 1.0 L/min (QC = 5 L/min) to 1.5 L/min (QC = 8 L/min) for SaO2 target = 90%. Corresponding differences of QEC for SaO2 target = 94% were 4.7 L/min and 7.9 L/min, respectively.
Conclusion: Bicaval drainage under ECMO via the IVC + SVC → RA route gave a superior systemic oxygenation performance when both QEC/QC and pulmonary shunt were high. The VV-V ECMO configuration (IVC + SVC → RA route) might be an attractive rescue strategy in case of refractory hypoxaemia under VV ECMO.
Keywords: Bicaval drainage; Oxygenation determinants; Oxygenation performance; Pulmonary shunt; Rescue therapy; Structural recirculation; Superior cava drainage; Superior cava shunt; Triple cannulation; VV-V configuration.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Schmidt M, Pham T, Arcadipane A, et al. Mechanical ventilation management during extracorporeal membrane oxygenation for acute respiratory distress syndrome. An international multicenter prospective cohort. Am J Respir Crit Care Med. 2019;200:1002–1012. doi: 10.1164/rccm.201806-1094OC. - DOI - PubMed
-
- Peek G, Mugford M, Tiruvoipati R, et al., CESAR trial collaboration (2009) Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): a multicentre randomised controlled trial. Lancet 374: 1351–1363. - PubMed
LinkOut - more resources
Full Text Sources
