

Validation of ultrasonography for measurement of cartilage thickness in the equine carpus
- PMID: 35347811
- PMCID: PMC9545370
- DOI: 10.1111/vru.13085
Validation of ultrasonography for measurement of cartilage thickness in the equine carpus
Abstract
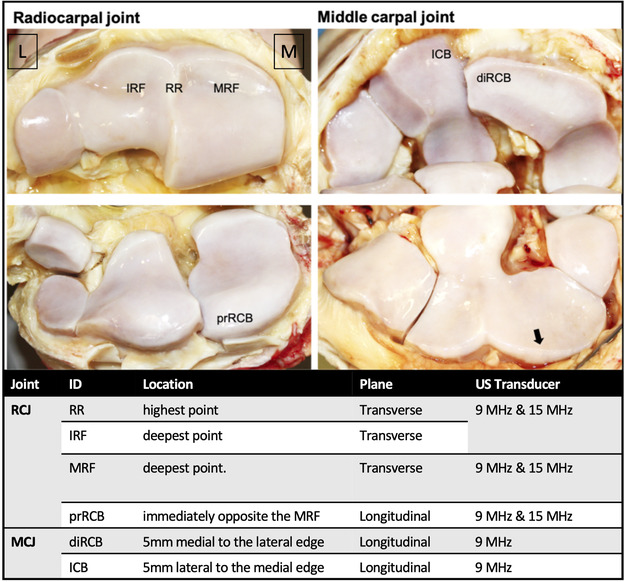
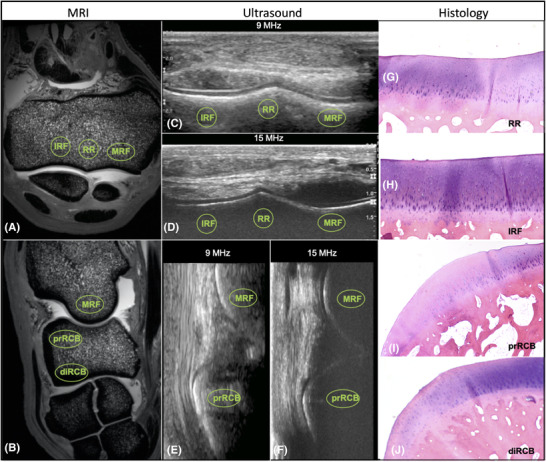
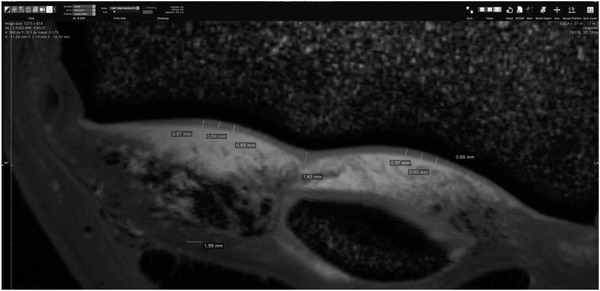
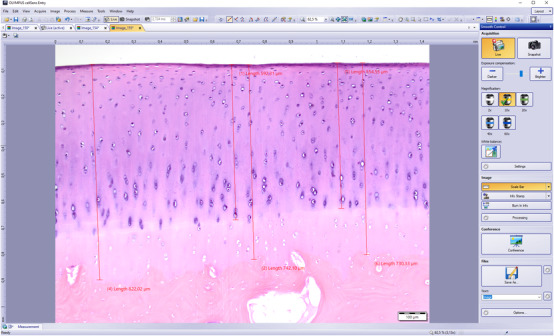
Articular cartilage thinning is an important hallmark of osteoarthritis (OA), and ultrasonography (US) is a clinically accessible tool potentially suitable for repeated evaluation. The aim of the present prospective methods comparison study was to validate US as a tool for measuring cartilage thickness in the carpus of the horse. Eight Standardbred trotters underwent US examination with 9 and 15 MHz linear transducers. Six anatomical locations in the radiocarpal joint (RCJ) and middle carpal joint (MCJ) were examined. The same joints were assessed by ultrahigh field (9.4 Tesla) magnetic resonance imaging (MRI) and histology. Associations between measurements obtained by the different modalities were assessed by ANOVA, Deming regression, Pearson correlation and Bland-Altman plots. Histologically assessed total cartilage thickness (the noncalcified cartilage (NCC) plus the calcified cartilage zone (CCZ)) overestimated thickness compared to MRI (P < 0.01) and US (P < 0.01). US 15 MHz had substantial agreement with MRI and NCC histology, and repeatability was acceptable (coefficient of variation = 8.6-17.9%) when used for assessment of cartilage thickness in the RCJ. In contrast, 9 MHz US showed poorer agreement with MRI and NCC histology, as it overestimated the thickness of thin cartilage and underestimated the thickness of thicker cartilage in the RCJ and MCJ. Moreover, repeatability was suboptimal (coefficient of variation = 10.4-26.3%). A 15 MHz transducer US is recommended for detecting changes in RCJ cartilage thickness or monitoring development over time, and it has the potential for noninvasive assessment of cartilage health in horses.
Keywords: front knee; histopathology; horse; orthopedic; ultrasound.
© 2022 The Authors. Veterinary Radiology & Ultrasound published by Wiley Periodicals LLC on behalf of American College of Veterinary Radiology.
Conflict of interest statement
The authors have declared no conflict of interest.
Figures




References
-
- Dyson PK, Jackson BF, Pfeiffer DU, Price JS. Days lost from training by two‐ and three‐year‐old Thoroughbred horses: a survey of seven UK training yards. Equine Vet J. 2008; 40(7):650‐657. - PubMed
-
- Schlueter AE, Orth MW. Equine osteoarthritis: a brief review of the disease and its causes. Equine Comp Exerc Physiol. 2004; 1(4):221‐231.
-
- Murray RC, Dyson SJ. EquineCarpus. 3th ed. Elsevier Inc; 2018;
-
- Ross MW. The Carpus. 2nd ed. Elsevier Inc; 2010;
-
- Goldring SR, Goldring MB. Changes in the osteochondral unit during osteoarthritis: structure, function and cartilage bone crosstalk. Nat Rev Rheumatol. 2016; 12(11):632‐644. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
