

The wide spectrum of cryoglobulinemic vasculitis and an overview of therapeutic advancements
- PMID: 35348938
- PMCID: PMC8960698
- DOI: 10.1007/s10238-022-00808-1
The wide spectrum of cryoglobulinemic vasculitis and an overview of therapeutic advancements
Abstract
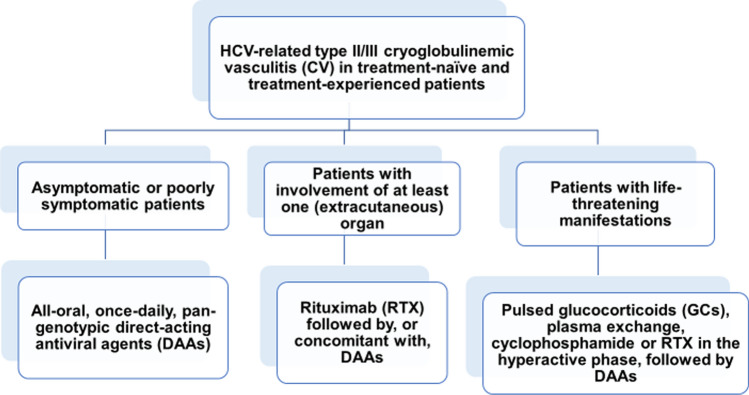
Immunoglobulins that reversibly precipitate at temperatures below 37 °C are called cryoglobulins (CGs). Cryoglobulinemia often manifests as cryoglobulinemic vasculitis (CV), whose symptoms range in severity from purpuric eruptions to life-threatening features. The majority of CV patients are infected with hepatitis C virus (HCV), whereas lymphoproliferative disorders or connective tissue diseases (CTD) are commonly diagnosed among patients with CV of non-infectious origin. In the absence of detectable associated disease, cryoglobulinemia is classified as "essential" (EMC). All HCV-positive CV patients should be given direct-acting antiviral agents (DAAs) that are consistently able to induce a sustained virologic response (SVR). Glucocorticoids (GCs) can mitigate CV-associated vasculitis, but they have no role as maintenance therapy. Cyclophosphamide restrains the hyperactive phase(s) of the disease and the post-apheresis rebound of newly synthesized CGs. Its use has been largely replaced by rituximab (RTX) in patients unresponsive to DAAs, patients progressing to B-cell non-Hodgkin lymphoma (B-NHL) and patients in whom CV persists or reappears after clearance of HCV. Therapeutic apheresis is an emergency treatment for CV patients with hyperviscosity syndrome. HCV-positive CV patients are at an increased risk of developing NHL, but the achievement of SVR can effectively prevent HCV-related NHL or induce the remission of an already established lymphoma, even without chemotherapy. The treatment of patients with IgM or IgG monoclonal cryoglobulins and an underlying immunoproliferative disorder is based on the regimens adopted for patients with the same B-cell malignancies but without circulating CGs. For patients with CTD, GCs plus alkylating agents or RTX are similarly effective as first-line therapy and in the relapse/refractory setting. In patients with EMC, treatment should consist of GCs plus RTX, with the dose of GCs tapered as soon as possible to reduce the risk of infectious complications.
Keywords: Cryoglobulin; Cryoglobulinemic vasculitis; Glucocorticoids; HCV; Non-Hodgkin lymphoma; Rituximab; Therapeutic apheresis.
© 2022. The Author(s), under exclusive licence to Springer Nature Switzerland AG.
Conflict of interest statement
The authors have no relevant financial or non-financial interests to disclose.
Figures



References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
