

This is a preprint.
Robust, persistent adaptive immune responses to SARS-CoV-2 in the oropharyngeal lymphoid tissue of children
- PMID: 35350206
- PMCID: PMC8963700
- DOI: 10.21203/rs.3.rs-1276578/v1
Robust, persistent adaptive immune responses to SARS-CoV-2 in the oropharyngeal lymphoid tissue of children
Update in
-
Adaptive immune responses to SARS-CoV-2 persist in the pharyngeal lymphoid tissue of children.Nat Immunol. 2023 Jan;24(1):186-199. doi: 10.1038/s41590-022-01367-z. Epub 2022 Dec 19. Nat Immunol. 2023. PMID: 36536106 Free PMC article.
Abstract
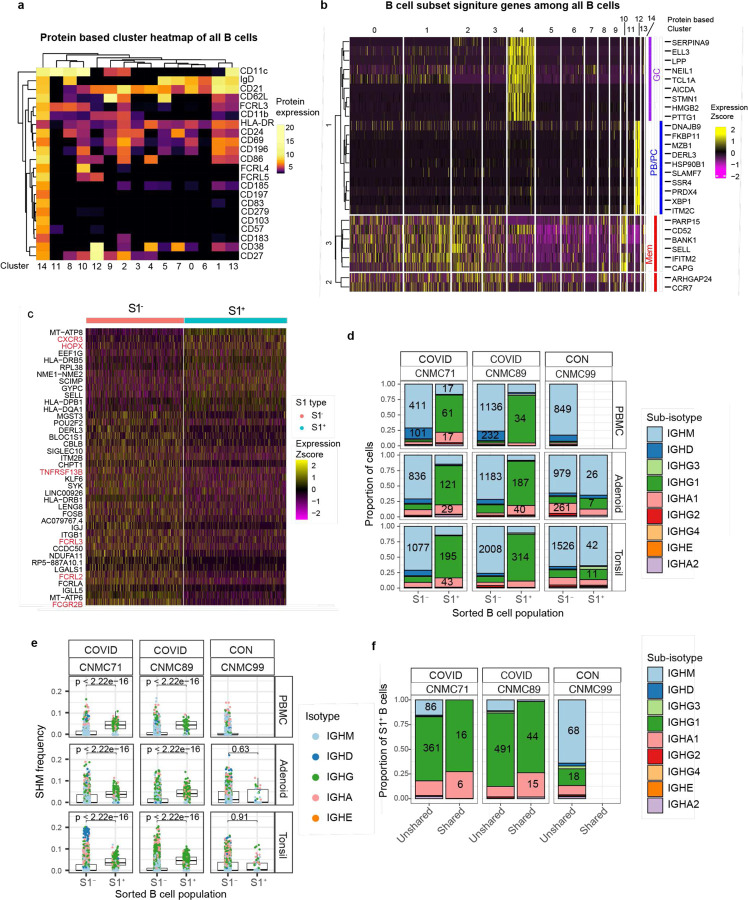
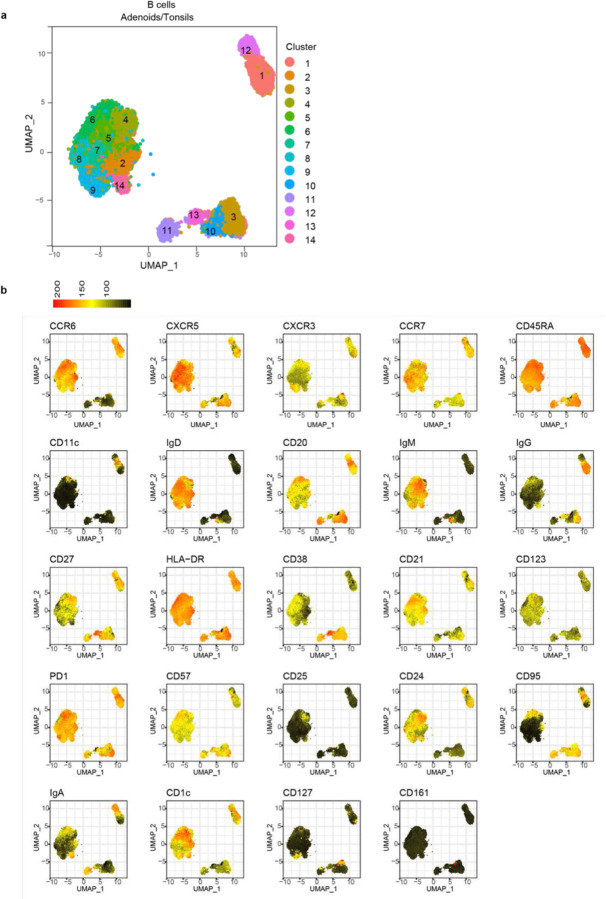
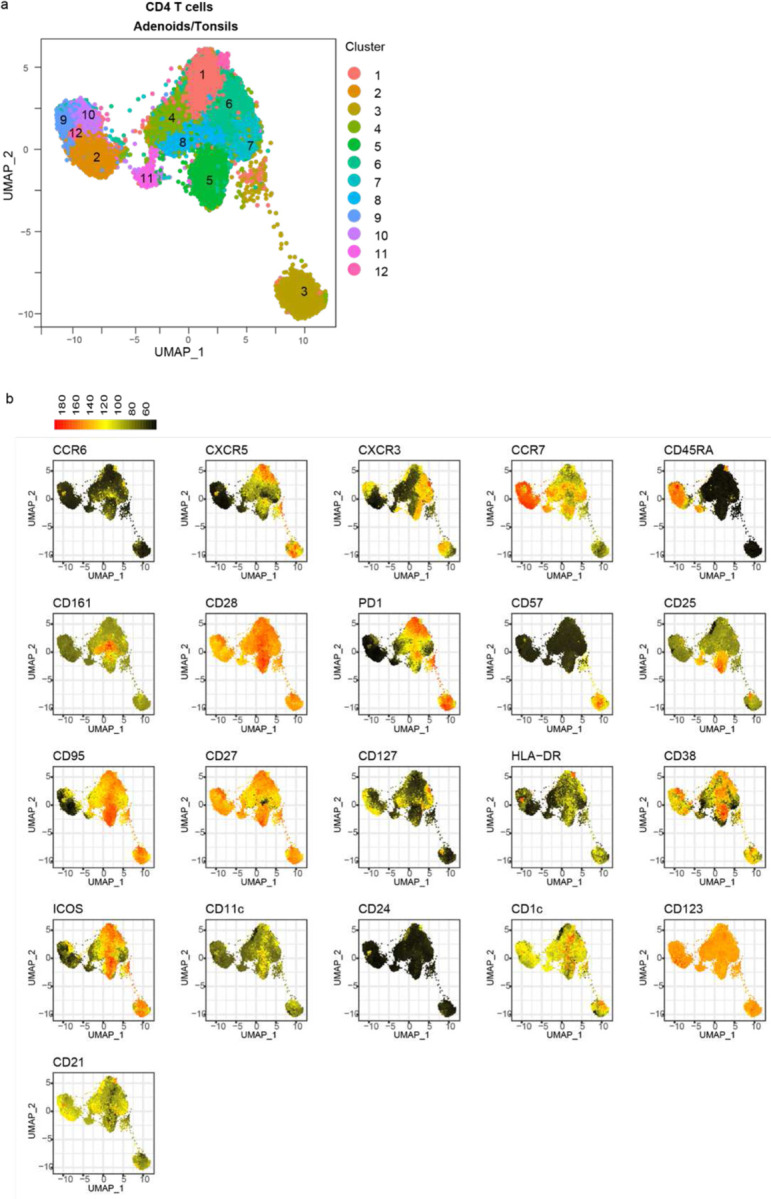
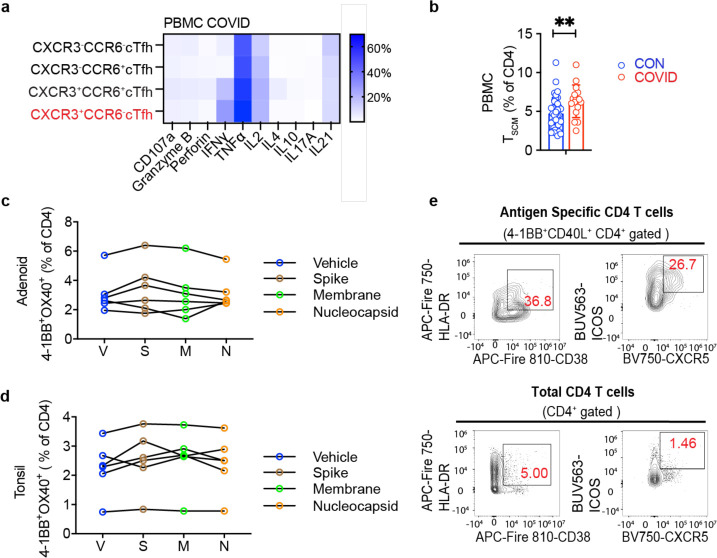
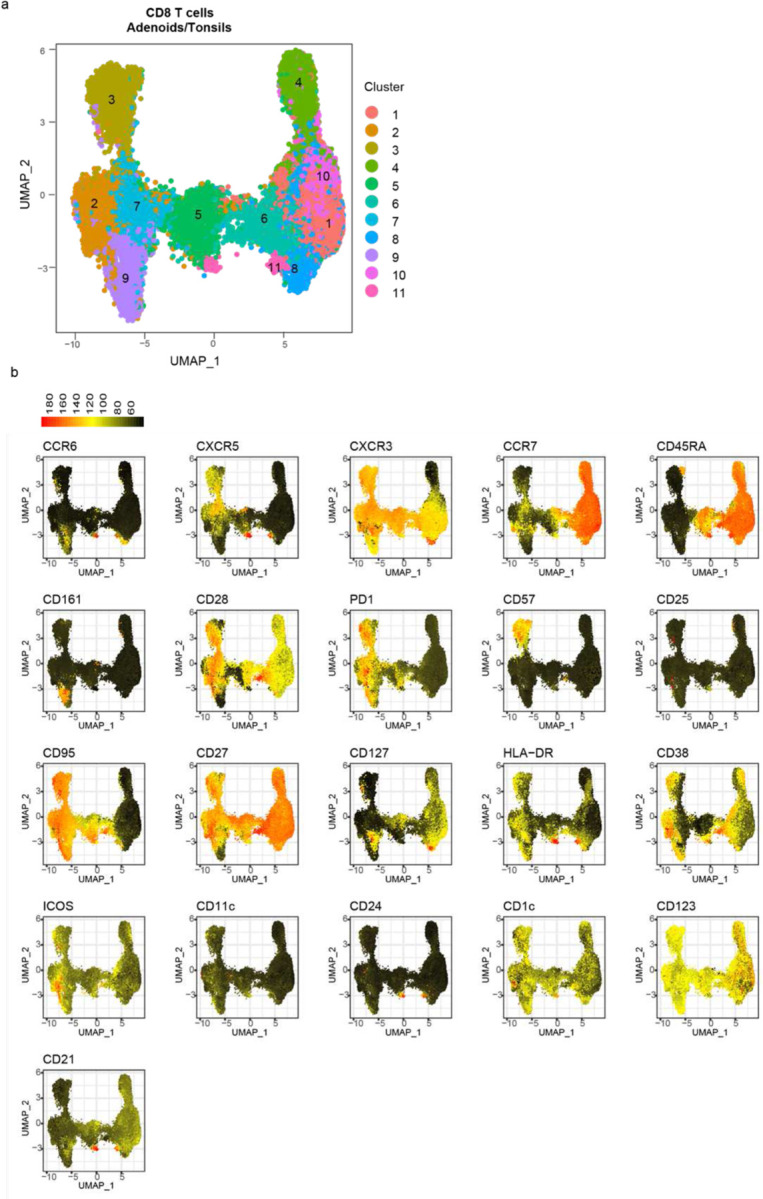
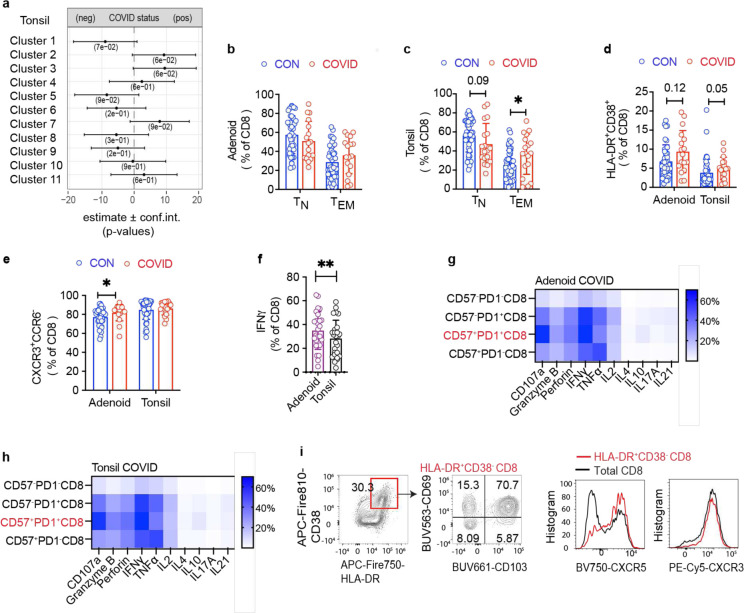
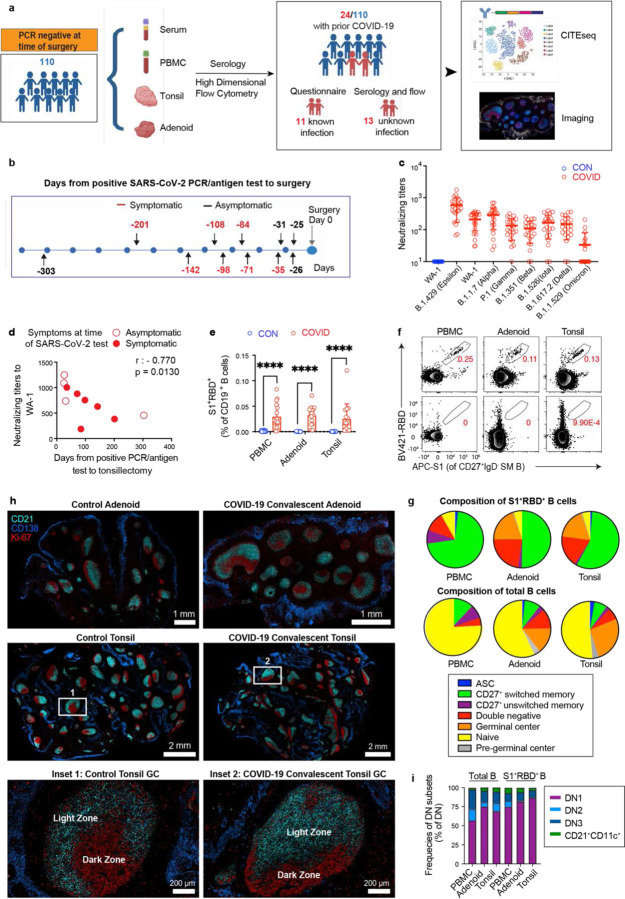
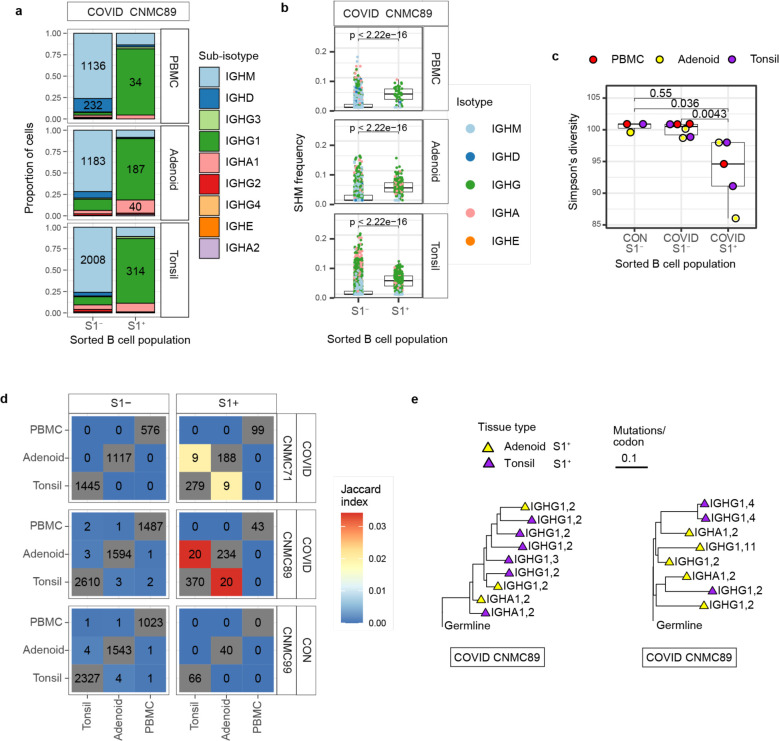
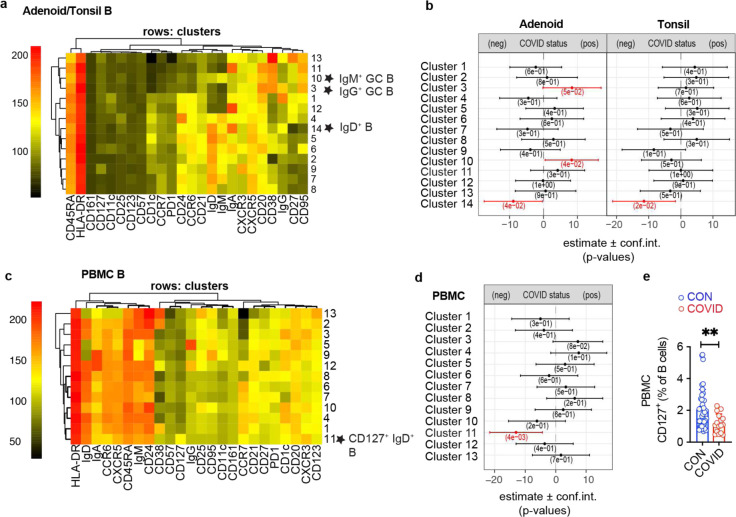
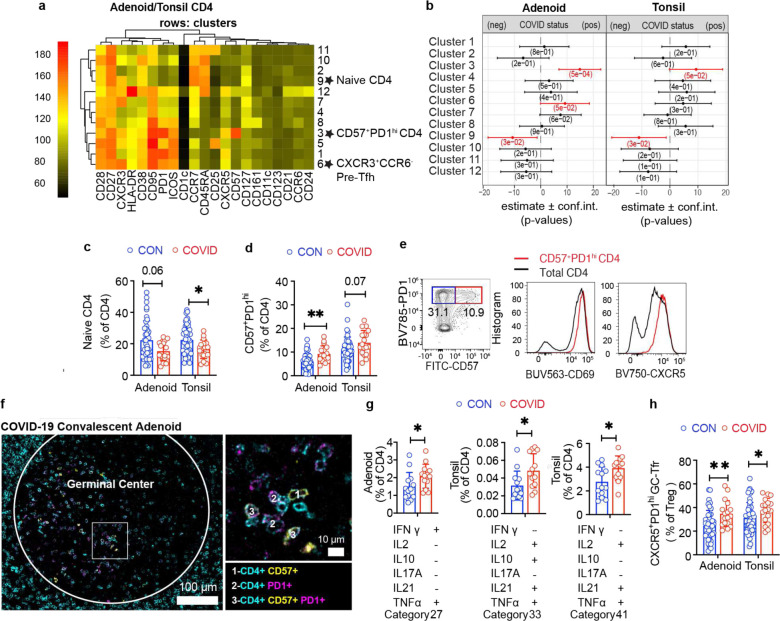
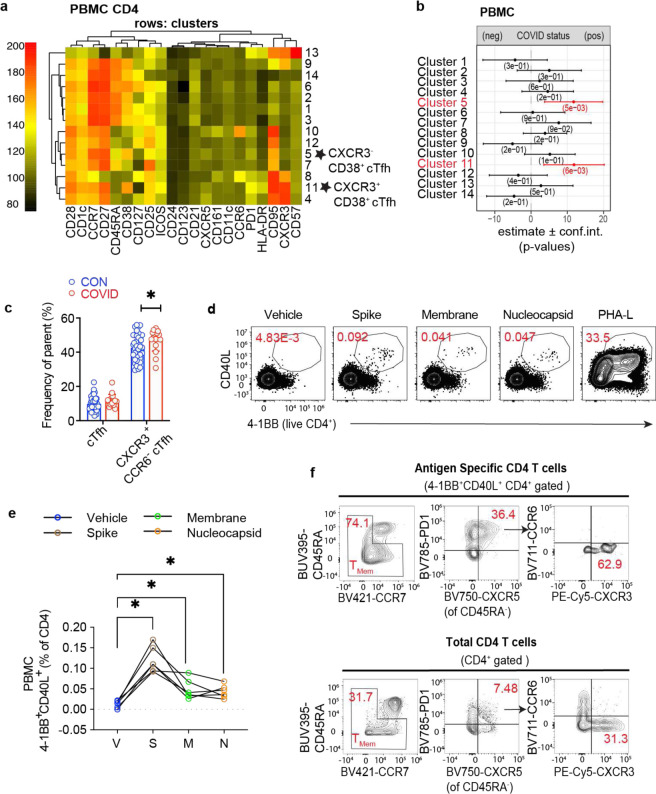
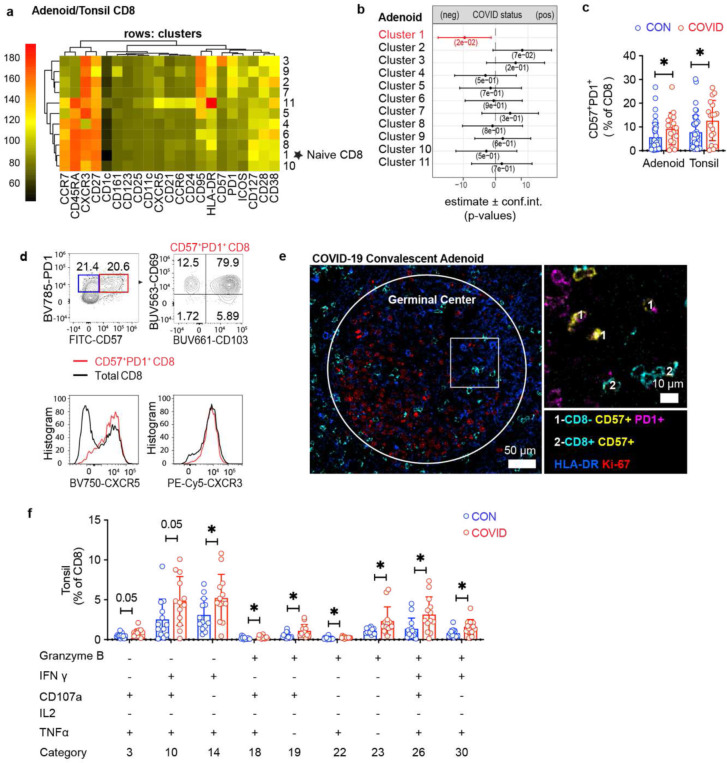
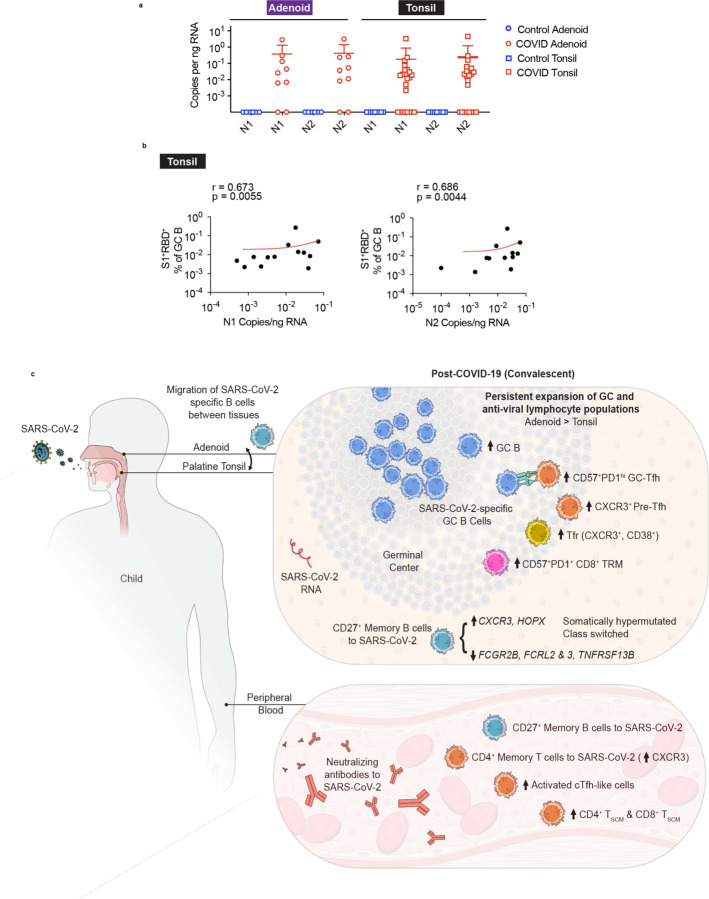
SARS-CoV-2 infection triggers adaptive immune responses from both T and B cells. However, most studies focus on peripheral blood, which may not fully reflect immune responses in lymphoid tissues at the site of infection. To evaluate both local and systemic adaptive immune responses to SARS-CoV-2, we collected peripheral blood, tonsils, and adenoids from 110 children undergoing tonsillectomy/adenoidectomy during the COVID-19 pandemic and found 24 with evidence of prior SARS-CoV-2 infection, including detectable neutralizing antibodies against multiple viral variants. We identified SARS-CoV-2-specific germinal center (GC) and memory B cells; single cell BCR sequencing showed that these virus-specific B cells were class-switched and somatically hypermutated, with overlapping clones in the adenoids and tonsils. Oropharyngeal tissues from COVID-19-convalescent children showed persistent expansion of GC and anti-viral lymphocyte populations associated with an IFN-γ-type response, with particularly prominent changes in the adenoids, as well as evidence of persistent viral RNA in both tonsil and adenoid tissues of many participants. Our results show robust, tissue-specific adaptive immune responses to SARS-CoV-2 in the upper respiratory tract of children weeks to months after acute infection, providing evidence of persistent localized immunity to this respiratory virus.
Conflict of interest statement
Figures





References
Main References:
Methods References:
-
- Zahra F. T., Bellusci L., Grubbs G., Golding H. & Khurana S. Neutralisation of circulating SARS-CoV-2 delta and omicron variants by convalescent plasma and SARS-CoV-2 hyperimmune intravenous human immunoglobulins for treatment of COVID-19. Annals of the Rheumatic Diseases, annrheumdis-2022–222115, doi: 10.1136/annrheumdis-2022-222115 (2022). - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
