

Analysis of Conjunctival Sac Microbiome in Dry Eye Patients With and Without Sjögren's Syndrome
- PMID: 35350577
- PMCID: PMC8957797
- DOI: 10.3389/fmed.2022.841112
Analysis of Conjunctival Sac Microbiome in Dry Eye Patients With and Without Sjögren's Syndrome
Abstract
Purpose: To analyze the conjunctival sac microbial communities in patients with Sjögren's syndrome-associated dry eyes (SSDE) and non-Sjögren's syndrome-associated dry eyes (NSSDE), compared with normal controls (NC).
Methods: Conjunctival sac swab samples from 23 eyes of SSDE, 36 eyes of NSSDE, and 39 eyes of NC were collected. The V3-V4 region of the 16S ribosomal RNA (rRNA) gene high-throughput sequencing was performed on an Illumina MiSeq platform and analyzed using Quantitative Insights Into Microbial Ecology (QIIME). Alpha diversity was employed to analyze microbiome diversity through Chao1 and Shannon indexes. Beta diversity was demonstrated by the principal coordinates analysis (PCoA) and Partial Least Squares Discrimination Analysis (PLS-DA). The relative abundance was bioinformatically analyzed at the phylum and genus levels.
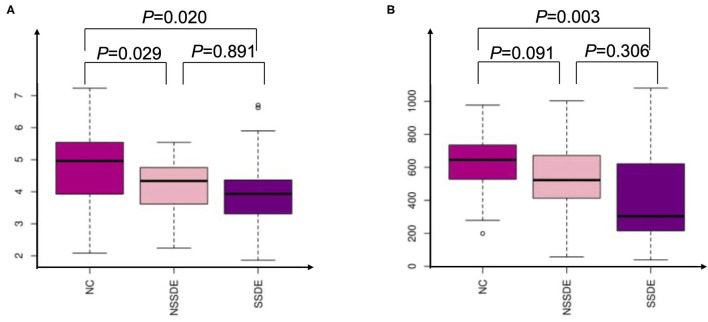
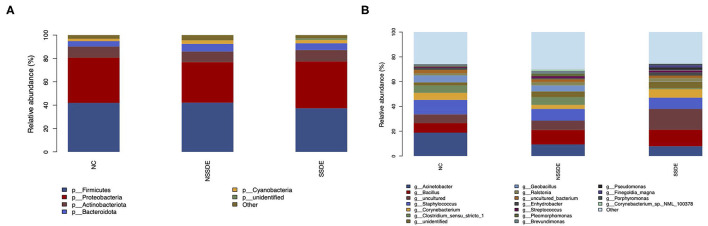
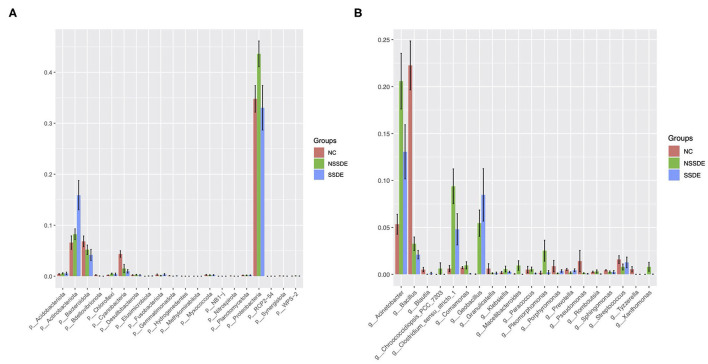
Results: The alpha diversity was lower in patients with dry eye disease (Shannon index: NC vs. SSDE: P = 0.020, NC vs. NSSDE: P = 0.029). The beta diversity showed divergent microbiome composition in different groups (NC vs. SSDE: P = 0.001, NC vs. NSSDE: P = 0.001, NSSDE vs. SSDE: P = 0.005). The top 5 abundant phyla were Firmicutes, Proteobacteria, Actinobacteriota, Bacteroidota, and Cyanobacteria in all three groups. The top five abundant genera included Acinetobacter, Staphylococcus, Bacillus, Corynebacterium, and Clostridium_sensu_stricto_1. The relative microbiome abundance was different between groups. The Firmicutes/Bacteroidetes (F/B) ratio was 6.42, 7.31, and 9.71 in the NC, NSSDE, and SSDE groups, respectively (NC vs. SSDE: P = 0.038, NC vs. NSSDE: P = 0.991, SSDE vs. NSSDE: P = 0.048).
Conclusion: The diversity of conjunctival sac microbiome in patients with NSSDE and SSDE was diminished compared with NC. The main microbiome at the phylum and genus level were similar between groups, but the relative abundance had variations. The Firmicutes/Bacteroidetes ratio was higher in the SSDE group.
Keywords: Sjögren's syndrome; dry eyes; microbial composition; microbial diversity; ocular surface.
Copyright © 2022 Song, Xiao, Chen and Long.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
LinkOut - more resources
Full Text Sources