

Bradykinin-induced angioedema in the emergency department
- PMID: 35350995
- PMCID: PMC8966254
- DOI: 10.1186/s12245-022-00408-6
Bradykinin-induced angioedema in the emergency department
Abstract
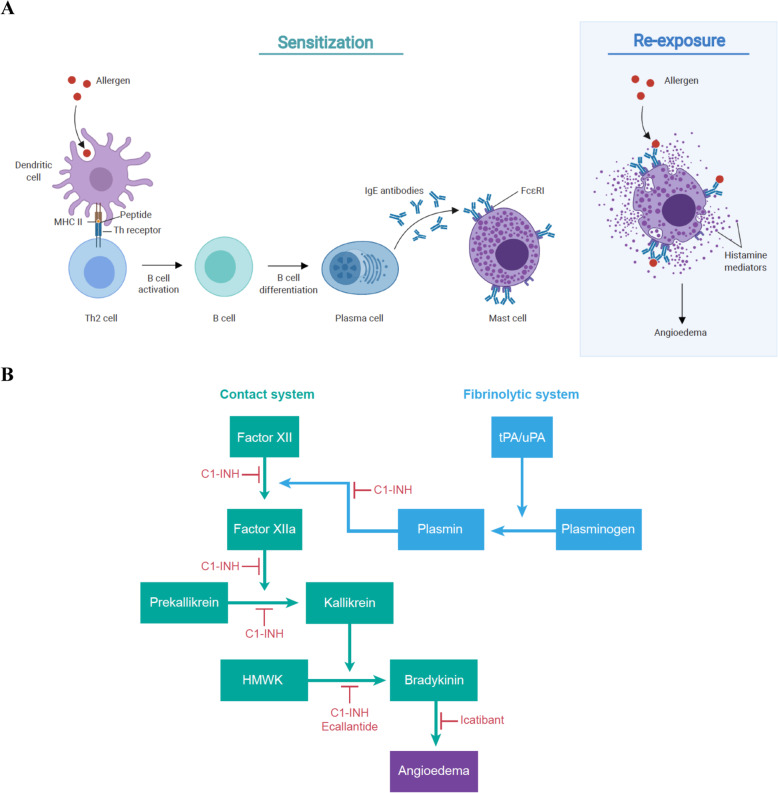
Background: Acute airway angioedema commonly occurs through two distinct mechanisms: histamine- and bradykinin-dependent. Although they respond to distinct treatments, these two potentially life-threatening states present similarly. Poor recognition of the bradykinin-dependent pathway leads to treatment errors in the emergency department (ED), despite the availability of multiple pharmacologic options for hereditary angioedema (HAE) and other forms of bradykinin-induced angioedema. Here, we consider the pathophysiology and clinical features of bradykinin-induced angioedema, and we present a systematic literature review exploring the effectiveness of the available therapies for managing such cases.
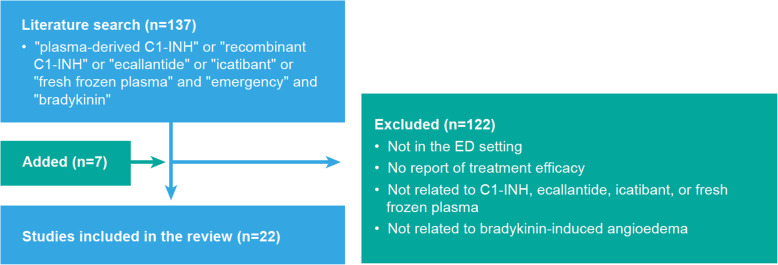
Methods: PubMed searches using 'emergency', 'bradykinin' and various therapeutic product names identified studies reporting the efficacy of treatments for bradykinin-induced angioedema in the ED setting. In all, 22 studies met prespecified criteria and are analysed here.
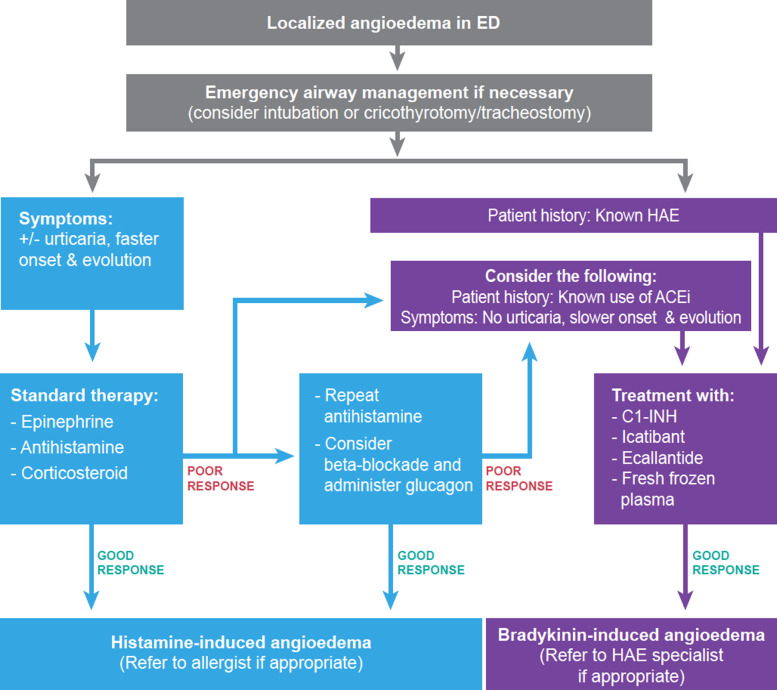
Findings: Whereas histamine-induced angioedema has a faster onset and often presents with urticaria, bradykinin-induced angioedema is slower in onset, with greater incidence of abdominal symptoms. Acute airway angioedema in the ED should initially be treated with anaphylactic protocols, focusing on airway management and treatment with epinephrine, antihistamine and systemic steroids. Bradykinin-induced angioedema should be considered if this standard treatment is not effective, despite proper dosing and regard of beta-adrenergic blockade. Therapeutics currently approved for HAE appear as promising options for this and other forms of bradykinin-induced angioedema encountered in the ED.
Conclusion: Diagnostic algorithms of bradykinin-induced angioedema should be followed in the ED, with early use of approved therapies to improve patient outcomes.
Keywords: Angioedema; Bradykinin; Emergency; Histamine.
© 2022. The Author(s).
Conflict of interest statement
Jacques Hébert reports personal fees outside the submitted work for advisory boards and teaching from Takeda and CSL Behring. Hugo Chapdelaine declares grants outside the submitted work from Takeda, CSL Behring, Pharvaris, Dyax, Green Cross, Sanofi, Merck and Novartis. He also reports personal fees outside the submitted work from CSL Behring, Takeda and Sobi. He is also an associate review editor with Frontiers in Immunology. Benoit Laramée declares participating in advisory committees or presentations from ALK, Takeda, CSL Behring, Novartis and Pedia-Pharm. Rémi Gagnon declares being a principal investigator on HAE trials funded by BioCryst, Takeda, CSL Behring and Pharvaris. No other competing interests were declared.
Figures
Similar articles
-
Recognition and Differential Diagnosis of Hereditary Angioedema in the Emergency Department.J Emerg Med. 2021 Jan;60(1):35-43. doi: 10.1016/j.jemermed.2020.09.044. Epub 2020 Nov 17. J Emerg Med. 2021. PMID: 33218838 Review.
-
Evaluation and Management of Angioedema in the Emergency Department.West J Emerg Med. 2019 Jul;20(4):587-600. doi: 10.5811/westjem.2019.5.42650. Epub 2019 Jul 2. West J Emerg Med. 2019. PMID: 31316698 Free PMC article. Review.
-
Management of angioedema without urticaria in the emergency department.Ann Med. 2014 Dec;46(8):607-18. doi: 10.3109/07853890.2014.949300. Ann Med. 2014. PMID: 25580506 Review.
-
A Comprehensive Review of Bradykinin-Induced Angioedema Versus Histamine-Induced Angioedema in the Emergency Department.Cureus. 2022 Nov 30;14(11):e32075. doi: 10.7759/cureus.32075. eCollection 2022 Nov. Cureus. 2022. PMID: 36600855 Free PMC article. Review.
-
Consequences of Misdiagnosed and Mismanaged Hereditary Angioedema Laryngeal Attacks: An Overview of Cases from the Romanian Registry.Case Rep Emerg Med. 2018 Oct 22;2018:6363787. doi: 10.1155/2018/6363787. eCollection 2018. Case Rep Emerg Med. 2018. PMID: 30425862 Free PMC article.
Cited by
-
Neurologic and Psychiatric Manifestations of Bradykinin-Mediated Angioedema: Old and New Challenges.Int J Mol Sci. 2023 Jul 29;24(15):12184. doi: 10.3390/ijms241512184. Int J Mol Sci. 2023. PMID: 37569559 Free PMC article. Review.
-
Deaths from Angioedema-Anaphylaxis and Covid-19.Acad Forensic Pathol. 2025 Feb 21:19253621251320212. doi: 10.1177/19253621251320212. Online ahead of print. Acad Forensic Pathol. 2025. PMID: 39991143 Free PMC article.
-
Hereditary Angioedema.Cureus. 2023 Jul 18;15(7):e42088. doi: 10.7759/cureus.42088. eCollection 2023 Jul. Cureus. 2023. PMID: 37602066 Free PMC article.
-
Life-Threatening tPA-Associated Angioedema: A Rare Case Report and Critical Review.Am J Case Rep. 2024 Sep 14;25:e944221. doi: 10.12659/AJCR.944221. Am J Case Rep. 2024. PMID: 39275799 Free PMC article. Review.
-
Bradykinin Metabolism and Drug-Induced Angioedema.Int J Mol Sci. 2023 Jul 19;24(14):11649. doi: 10.3390/ijms241411649. Int J Mol Sci. 2023. PMID: 37511409 Free PMC article. Review.
References
-
- Jaiganesh T, Wiese M, Hollingsworth J, Hughan C, Kamara M, Wood P, et al. Acute angioedema: recognition and management in the emergency department. Eur J Emerg Med. 2013;20(1):10–17. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
