

Mortuary and hospital-based HIV mortality surveillance among decedents in a low-resource setting: lessons from Western Kenya
- PMID: 35351057
- PMCID: PMC8962591
- DOI: 10.1186/s12889-022-12909-3
Mortuary and hospital-based HIV mortality surveillance among decedents in a low-resource setting: lessons from Western Kenya
Abstract
Background: Lack of dependable morbidity and mortality data complicates efforts to measure the demographic or population-level impact of the global HIV/AIDS epidemic. Mortuary-based mortality surveillance can address gaps in vital statistics in low-resource settings by improving accuracy of measuring HIV-associated mortality and indicators of access to treatment services among decedents. This paper describes the process and considerations taken in conducting mortuary and hospital-based HIV mortality surveillance among decedents in Kenya.
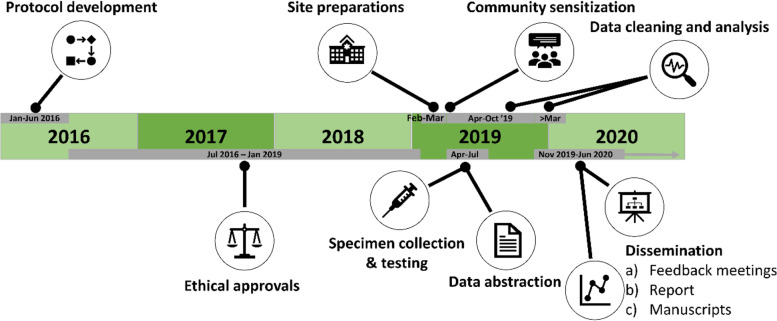
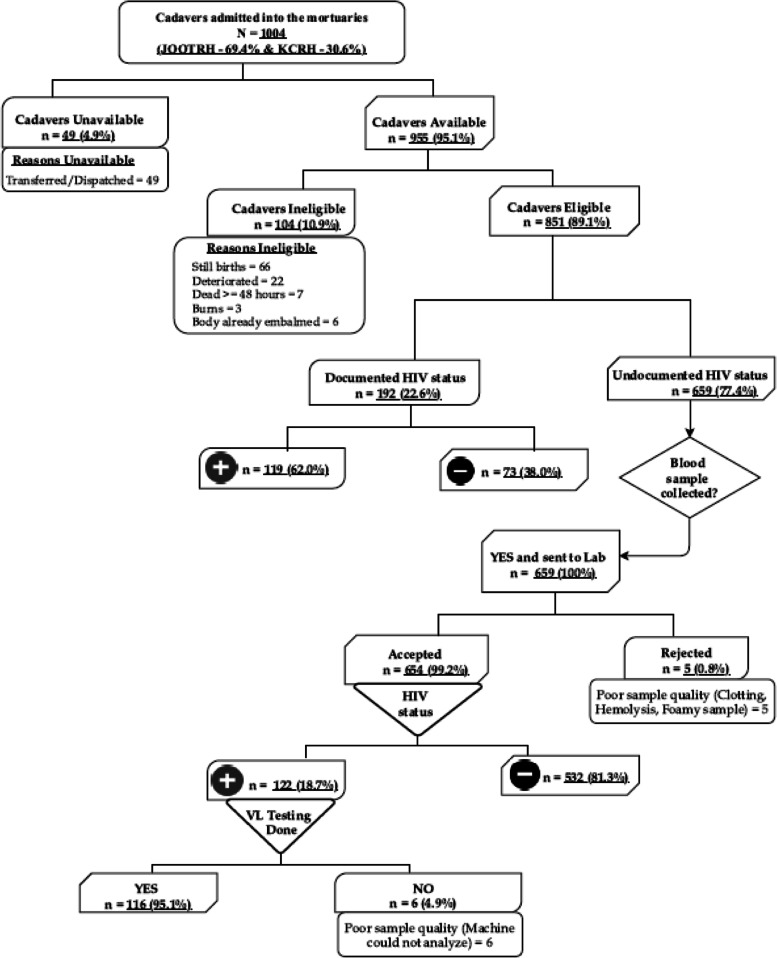
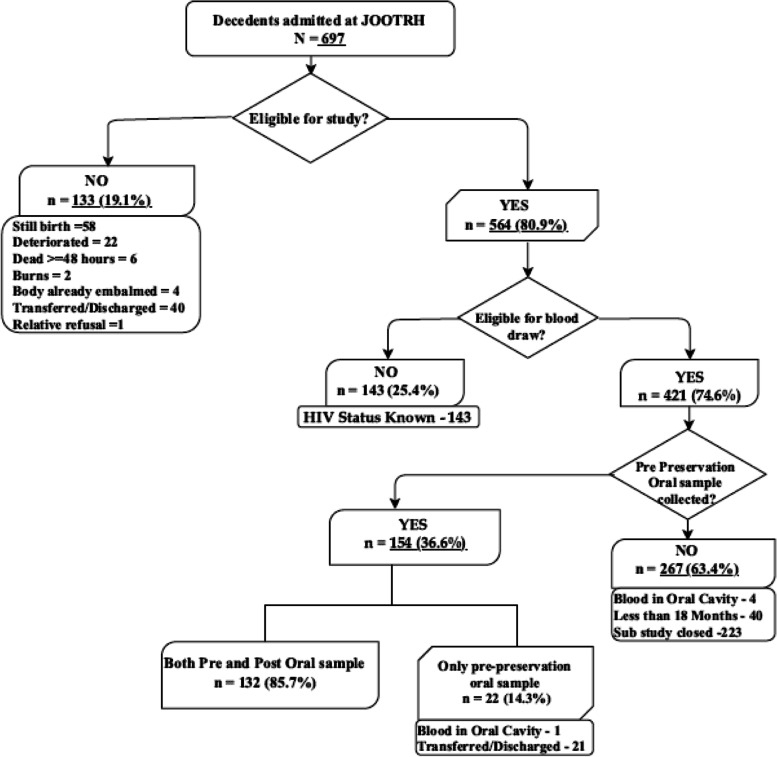
Main text: We conducted HIV mortuary and hospital-based mortality surveillance at two of the largest mortuaries in Kisumu County, Kenya (April 16-July 12, 2019). Medical charts were reviewed for documentation of HIV status among eligible decedents. HIV testing was done on blood and oral fluid samples from decedents with undocumented HIV status and those whose medical records indicated HIV-negative test results > 3 months before death. A panel of experts established the cause of death according to the International Classification of Diseases, 10th Revision rules. Civil registry data for the year 2017 were abstracted and coded to corresponding ICD-10 codes. Of the 1004 decedents admitted to the two mortuaries during the study period, 49 (4.9%) were unavailable because they had been transferred to other facilities or dispatched for burial before enrolment. Of the 955 available decedents, 104 (10.9%) were ineligible for the study. Blood samples were collected from 659 (77.4%) decedents, and 654 (99.2%) were tested for HIV. Of the 564 decedents eligible for the OraQuick® validation sub-study, 154 were eligible for oral sample collection, and 132 (85.7%) matched pre- and post-embalming oral samples were collected and tested. Of the 851 eligible decedents, 241 (28.3%) had evidence of HIV infection: 119 had a diagnosis of HIV infection recorded in their patient files, and 122 had serological evidence of HIV infection.
Conclusion: This study shows that in low-resource settings, conducting hospital and mortuary-based surveillance is feasible and can be an alternative source of mortality data when civil registry data are inadequate.
Keywords: Decedents; HIV; Hospital-based; Lessons; Mortality; Mortuary; Surveillance.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- International Development Research Centre (Canada). Population and health in developing countries. Volume 1. Population, health, and survival at INDEPTH sites. v. 1. Ottawa: International Development Research Centre; 2002.
-
- Smith AL, Smith A, Gebrekidan TA, Mazive E, Nalishebo S, Sikanyiti P, et al. Mortality surveillance practices for measuring the demographic impact of HIV/AIDS in sub-Saharan Africa. jHASE. 2010; . Available from: https://www.researchgate.net/publication/260075303_Mortality_surveillanc....
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
