

Effects of patient-level risk factors, departmental allocation and seasonality on intrahospital patient transfer patterns: network analysis applied on a Norwegian single-centre data set
- PMID: 35351711
- PMCID: PMC8966550
- DOI: 10.1136/bmjopen-2021-054545
Effects of patient-level risk factors, departmental allocation and seasonality on intrahospital patient transfer patterns: network analysis applied on a Norwegian single-centre data set
Abstract
Objectives: Describe patient transfer patterns within a large Norwegian hospital. Identify risk factors associated with a high number of transfers. Develop methods to monitor intrahospital patient flows to support capacity management and infection control.
Design: Retrospective observational study of linked clinical data from electronic health records.
Setting: Tertiary care university hospital in the Greater Oslo Region, Norway.
Participants: All adult (≥18 years old) admissions to the gastroenterology, gastrointestinal surgery, neurology and orthopaedics departments at Akershus University Hospital, June 2018 to May 2019.
Methods: Network analysis and graph theory. Poisson regression analysis.
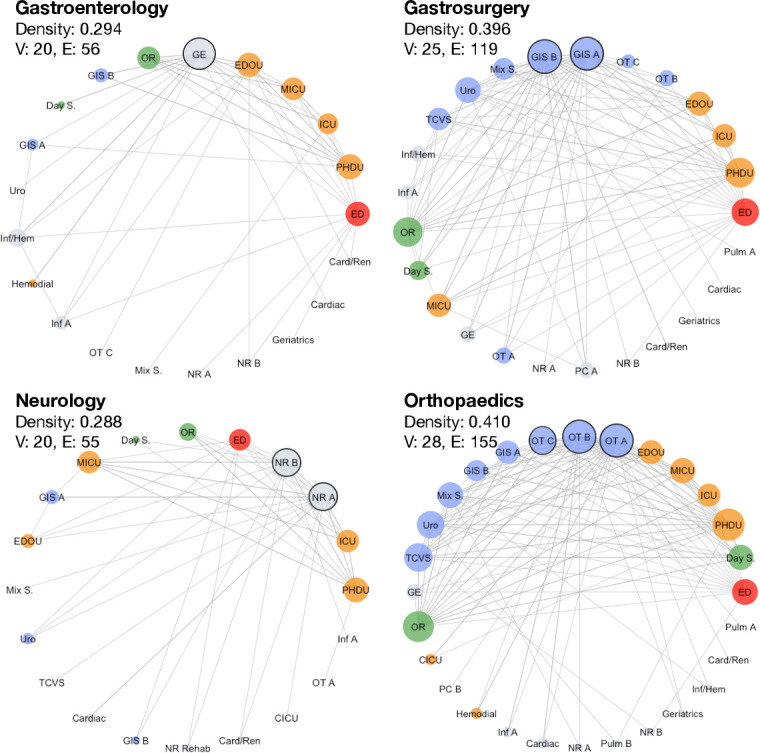
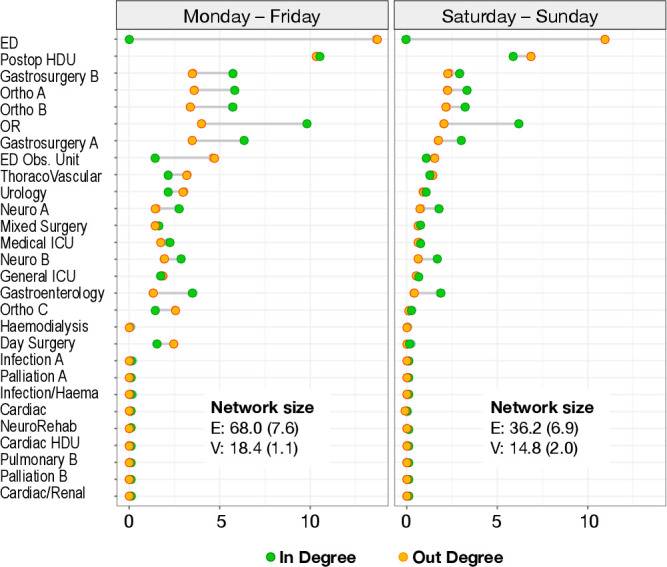
Outcome measures: Primary outcome was network characteristics at the departmental level. We describe location-to-location transfers using unweighted, undirected networks for a full-year study period. Weekly networks reveal changes in network size, density and key categories of transfers over time. Secondary outcome was transfer trajectories at the individual patient level. We describe the distribution of transfer trajectories in the cohort and associate number of transfers with patient clinical characteristics.
Results: The cohort comprised 17 198 hospital stays. Network analysis demonstrated marked heterogeneity across departments and throughout the year. The orthopaedics department had the largest transfer network size and density and greatest temporal variation. More transfers occurred during weekdays than weekends. Summer holiday affected transfers of different types (Emergency department-Any location/Bed ward-Bed ward/To-From Technical wards) differently. Over 75% of transferred patients followed one of 20 common intrahospital trajectories, involving one to three transfers. Higher number of intrahospital transfers was associated with emergency admission (transfer rate ratio (RR)=1.827), non-prophylactic antibiotics (RR=1.108), surgical procedure (RR=2.939) and stay in intensive care unit or high-dependency unit (RR=2.098). Additionally, gastrosurgical (RR=1.211), orthopaedic (RR=1.295) and neurological (RR=1.114) patients had higher risk of many transfers than gastroenterology patients (all effects: p<0.001).
Conclusions: Network and transfer chain analysis applied on patient location data revealed logistic and clinical associations highly relevant for hospital capacity management and infection control.
Keywords: health informatics; information management; organisation of health services; risk management.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures

Similar articles
-
Intrahospital transfers and adverse patient outcomes: An analysis of administrative health data.J Clin Nurs. 2017 Dec;26(23-24):4927-4935. doi: 10.1111/jocn.13976. Epub 2017 Oct 10. J Clin Nurs. 2017. PMID: 28748563
-
Assessment of Hospital Characteristics and Interhospital Transfer Patterns of Adults With Emergency General Surgery Conditions.JAMA Netw Open. 2021 Sep 1;4(9):e2123389. doi: 10.1001/jamanetworkopen.2021.23389. JAMA Netw Open. 2021. PMID: 34468755 Free PMC article.
-
Association between intrahospital transfer and hospital-acquired infection in the elderly: a retrospective case-control study in a UK hospital network.BMJ Qual Saf. 2021 Jun;30(6):457-466. doi: 10.1136/bmjqs-2020-012124. Epub 2021 Jan 25. BMJ Qual Saf. 2021. PMID: 33495288 Free PMC article.
-
Emergency rural obstetric transfers in South Australia: a review of the clinical and precipitating factors.Rural Remote Health. 2019 Feb;19(1):4634. doi: 10.22605/RRH4634. Epub 2019 Feb 6. Rural Remote Health. 2019. PMID: 30721624
-
Evaluating mental health decision units in acute care pathways (DECISION): a quasi-experimental, qualitative and health economic evaluation.Health Soc Care Deliv Res. 2023 Dec;11(25):1-221. doi: 10.3310/PBSM2274. Health Soc Care Deliv Res. 2023. PMID: 38149657
Cited by
-
Modular structures and the delivery of inpatient care in hospitals: a Network Science perspective on healthcare function and dysfunction.BMC Health Serv Res. 2022 Dec 10;22(1):1503. doi: 10.1186/s12913-022-08865-8. BMC Health Serv Res. 2022. PMID: 36494814 Free PMC article.
-
The impact of atypical intrahospital transfers on patient outcomes: a mixed methods study.Sci Rep. 2023 Sep 18;13(1):15417. doi: 10.1038/s41598-023-41966-w. Sci Rep. 2023. PMID: 37723183 Free PMC article.
-
Repercussions of moving patients on the context of practice: perspectives of the nursing team.Rev Lat Am Enfermagem. 2024 Mar 15;32:e4113. doi: 10.1590/1518-8345.7042.4113. eCollection 2024. Rev Lat Am Enfermagem. 2024. PMID: 38511734 Free PMC article.
-
A Scoping Review of Multilevel Patient-Sharing Network Measures in Health Services Research.Med Care Res Rev. 2025 Jun;82(3):203-224. doi: 10.1177/10775587241304140. Epub 2024 Dec 30. Med Care Res Rev. 2025. PMID: 40271968 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical