

The impact of pre-existing hypertension and its treatment on outcomes in patients admitted to hospital with COVID-19
- PMID: 35352027
- PMCID: PMC8963889
- DOI: 10.1038/s41440-022-00893-5
The impact of pre-existing hypertension and its treatment on outcomes in patients admitted to hospital with COVID-19
Abstract
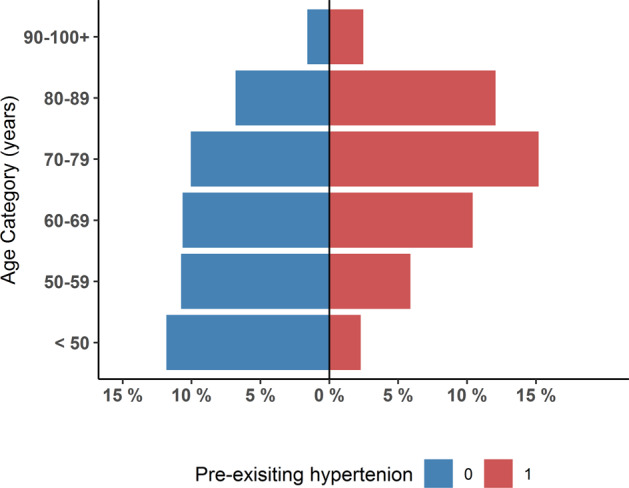
The impact of pre-existing hypertension on outcomes in patients with the novel corona virus (SARS-CoV-2) remains controversial. To address this, we examined the impact of pre-existing hypertension and its treatment on in-hospital mortality in patients admitted to hospital with Covid-19. Using the CAPACITY-COVID patient registry we examined the impact of pre-existing hypertension and guideline-recommended treatments for hypertension on in-hospital mortality in unadjusted and multi-variate-adjusted analyses using logistic regression. Data from 9197 hospitalised patients with Covid-19 (median age 69 [IQR 57-78] years, 60.6% male, n = 5573) was analysed. Of these, 48.3% (n = 4443) had documented pre-existing hypertension. Patients with pre-existing hypertension were older (73 vs. 62 years, p < 0.001) and had twice the occurrence of any cardiac disease (49.3 vs. 21.8%; p < 0.001) when compared to patients without hypertension. The most documented class of anti-hypertensive drugs were angiotensin receptor blockers (ARB) or angiotensin converting enzyme inhibitors (ACEi) (n = 2499, 27.2%). In-hospital mortality occurred in (n = 2020, 22.0%), with more deaths occurring in those with pre-existing hypertension (26.0 vs. 18.2%, p < 0.001). Pre-existing hypertension was associated with in-hospital mortality in unadjusted analyses (OR 1.57, 95% CI 1.42,1.74), no significant association was found following multivariable adjustment for age and other hypertension-related covariates (OR 0.97, 95% CI 0.87,1.10). Use of ACEi or ARB tended to have a protective effect for in-hospital mortality in fully adjusted models (OR 0.88, 95% CI 0.78,0.99). After appropriate adjustment for confounding, pre-existing hypertension, or treatment for hypertension, does not independently confer an increased risk of in-hospital mortality patients hospitalized with Covid-19.
Keywords: COVID-19; Hypertension; Public health; SARS-Cov-2.
© 2022. The Author(s).
Conflict of interest statement
BW has received honoraria for lectures on hypertension at medical/scientific meetings supported by Daiichi Sankyo, Pfizer, Menarini, Novartis, Boehringer Ingelheim, Servier. All other authors have nothing to declare.
Figures

Comment in
-
Severe COVID-19 and preexisting hypertension: a matter of age?Hypertens Res. 2022 Sep;45(9):1523-1525. doi: 10.1038/s41440-022-00978-1. Epub 2022 Jul 15. Hypertens Res. 2022. PMID: 35840751 Free PMC article. No abstract available.
References
-
- Sun Y, Guan X, Jia L, Xing N, Cheng L, Liu B, et al. Independent and combined effects of hypertension and diabetes on clinical outcomes in patients with COVID-19: A retrospective cohort study of Huoshen Mountain Hospital and Guanggu Fangcang Shelter Hospital. J Clin Hypertens (Greenwich) 2021;23:218–31. doi: 10.1111/jch.14146. - DOI - PMC - PubMed
-
- Kanwal A, Agarwala A, Warsinger-Martin L, Handberg EM COVID 19 and Hypertension: What we know and what we don’t know: ACC; 2020 [Available from: https://www.acc.org/latest-in-cardiology/articles/2020/07/06/08/15/covid....
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
