

Amyloid pathology but not APOE ε4 status is permissive for tau-related hippocampal dysfunction
- PMID: 35352105
- PMCID: PMC9128811
- DOI: 10.1093/brain/awab405
Amyloid pathology but not APOE ε4 status is permissive for tau-related hippocampal dysfunction
Abstract
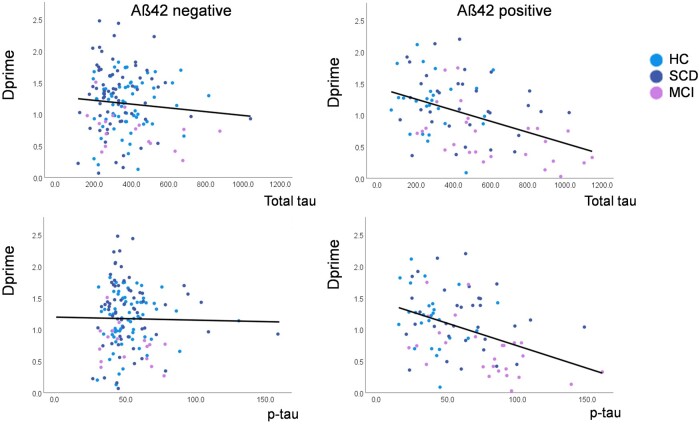
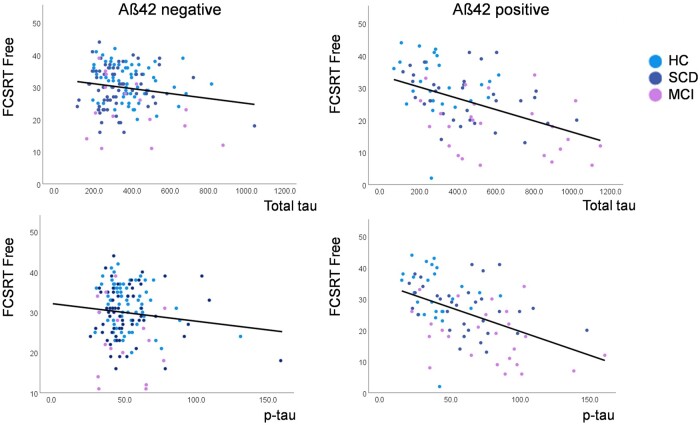
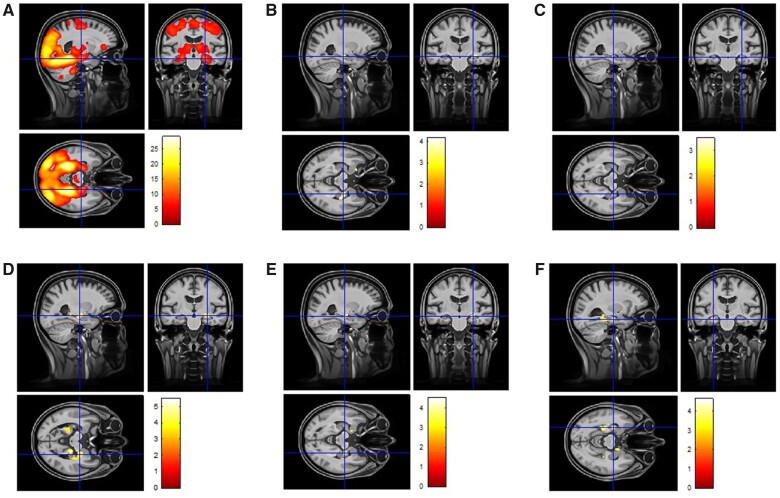
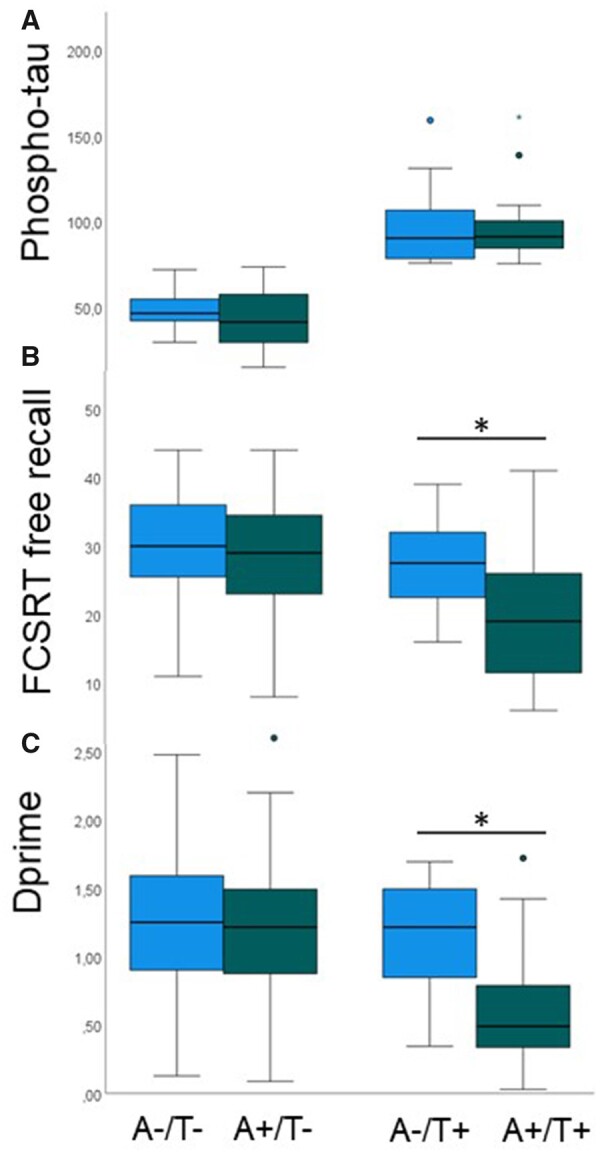
We investigated whether the impact of tau-pathology on memory performance and on hippocampal/medial temporal memory function in non-demented individuals depends on the presence of amyloid pathology, irrespective of diagnostic clinical stage. We conducted a cross-sectional analysis of the observational, multicentric DZNE-Longitudinal Cognitive Impairment and Dementia Study (DELCODE). Two hundred and thirty-five participants completed task functional MRI and provided CSF (92 cognitively unimpaired, 100 experiencing subjective cognitive decline and 43 with mild cognitive impairment). Presence (A+) and absence (A-) of amyloid pathology was defined by CSF amyloid-β42 (Aβ42) levels. Free recall performance in the Free and Cued Selective Reminding Test, scene recognition memory accuracy and hippocampal/medial temporal functional MRI novelty responses to scene images were related to CSF total-tau and phospho-tau levels separately for A+ and A- individuals. We found that total-tau and phospho-tau levels were negatively associated with memory performance in both tasks and with novelty responses in the hippocampus and amygdala, in interaction with Aβ42 levels. Subgroup analyses showed that these relationships were only present in A+ and remained stable when very high levels of tau (>700 pg/ml) and phospho-tau (>100 pg/ml) were excluded. These relationships were significant with diagnosis, age, education, sex, assessment site and Aβ42 levels as covariates. They also remained significant after propensity score based matching of phospho-tau levels across A+ and A- groups. After classifying this matched sample for phospho-tau pathology (T-/T+), individuals with A+/T+ were significantly more memory-impaired than A-/T+ despite the fact that both groups had the same amount of phospho-tau pathology. ApoE status (presence of the E4 allele), a known genetic risk factor for Alzheimer's disease, did not mediate the relationship between tau pathology and hippocampal function and memory performance. Thus, our data show that the presence of amyloid pathology is associated with a linear relationship between tau pathology, hippocampal dysfunction and memory impairment, although the actual severity of amyloid pathology is uncorrelated. Our data therefore indicate that the presence of amyloid pathology provides a permissive state for tau-related hippocampal dysfunction and hippocampus-dependent recognition and recall impairment. This raises the possibility that in the predementia stage of Alzheimer's disease, removing the negative impact of amyloid pathology could improve memory and hippocampal function even if the amount of tau-pathology in CSF is not changed, whereas reducing increased CSF tau-pathology in amyloid-negative individuals may not proportionally improve memory function.
Keywords: Alzheimer’s disease biomarker; hippocampus; memory; mild cognitive impairment; subjective cognitive decline.
© The Author(s) (2022). Published by Oxford University Press on behalf of the Guarantors of Brain.
Figures
Similar articles
-
Apolipoprotein E genotype and the diagnostic accuracy of cerebrospinal fluid biomarkers for Alzheimer disease.JAMA Psychiatry. 2014 Oct;71(10):1183-91. doi: 10.1001/jamapsychiatry.2014.1060. JAMA Psychiatry. 2014. PMID: 25162367
-
CSF total tau levels are associated with hippocampal novelty irrespective of hippocampal volume.Alzheimers Dement (Amst). 2018 Nov 2;10:782-790. doi: 10.1016/j.dadm.2018.10.003. eCollection 2018. Alzheimers Dement (Amst). 2018. PMID: 30555890 Free PMC article.
-
Alzheimer's pathology targets distinct memory networks in the ageing brain.Brain. 2019 Aug 1;142(8):2492-2509. doi: 10.1093/brain/awz154. Brain. 2019. PMID: 31199481 Free PMC article.
-
Characterizing the preclinical stages of Alzheimer's disease and the prospect of presymptomatic intervention.J Alzheimers Dis. 2013;33 Suppl 1(0 1):S405-16. doi: 10.3233/JAD-2012-129026. J Alzheimers Dis. 2013. PMID: 22695623 Free PMC article. Review.
-
Unraveling the Potential Underlying Mechanisms of Mild Behavioral Impairment: Focusing on Amyloid and Tau Pathology.Cells. 2024 Jul 8;13(13):1164. doi: 10.3390/cells13131164. Cells. 2024. PMID: 38995015 Free PMC article. Review.
Cited by
-
Single-value brain activity scores reflect both severity and risk across the Alzheimer's continuum.Brain. 2024 Nov 4;147(11):3789-3803. doi: 10.1093/brain/awae149. Brain. 2024. PMID: 38743817 Free PMC article.
-
Inhibitory temporo-parietal effective connectivity is associated with explicit memory performance in older adults.iScience. 2023 Aug 29;26(10):107765. doi: 10.1016/j.isci.2023.107765. eCollection 2023 Oct 20. iScience. 2023. PMID: 37744028 Free PMC article.
-
Cerebrospinal fluid reference proteins increase accuracy and interpretability of biomarkers for brain diseases.Nat Commun. 2024 May 1;15(1):3676. doi: 10.1038/s41467-024-47971-5. Nat Commun. 2024. PMID: 38693142 Free PMC article.
-
Beta-Amyloid and Its Asp7 Isoform: Morphological and Aggregation Properties and Effects of Intracerebroventricular Administration.Brain Sci. 2024 Oct 21;14(10):1042. doi: 10.3390/brainsci14101042. Brain Sci. 2024. PMID: 39452054 Free PMC article.
-
The relationship between resting-state amplitude fluctuations and memory-related deactivations of the default mode network in young and older adults.Hum Brain Mapp. 2023 Jun 15;44(9):3586-3609. doi: 10.1002/hbm.26299. Epub 2023 Apr 13. Hum Brain Mapp. 2023. PMID: 37051727 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
