

Deep learning for prediction of hepatocellular carcinoma recurrence after resection or liver transplantation: a discovery and validation study
- PMID: 35352293
- PMCID: PMC9174321
- DOI: 10.1007/s12072-022-10321-y
Deep learning for prediction of hepatocellular carcinoma recurrence after resection or liver transplantation: a discovery and validation study
Abstract
Background: There is a growing need for new improved classifiers of prognosis in hepatocellular carcinoma (HCC) patients to stratify them effectively.
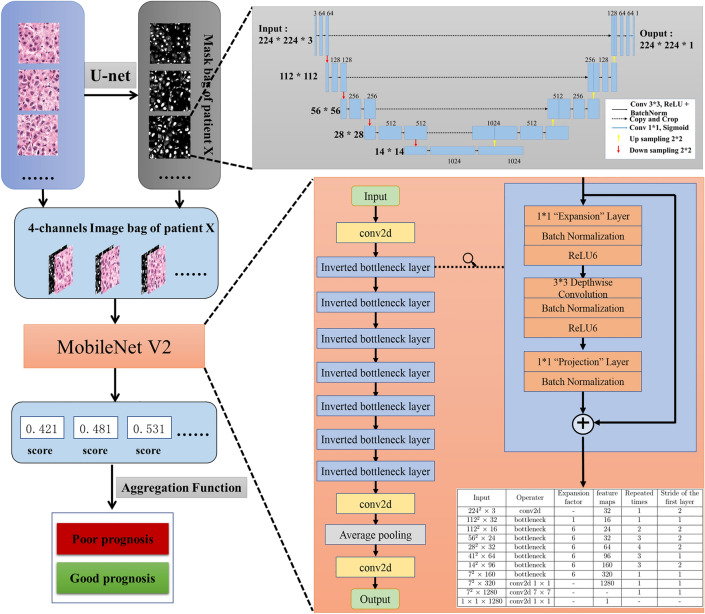
Methods: A deep learning model was developed on a total of 1118 patients from 4 independent cohorts. A nucleus map set (n = 120) was used to train U-net to capture the nuclear architecture. The training set (n = 552) included HCC patients that had been treated by resection. The liver transplantation (LT) set (n = 144) contained patients with HCC that had been treated by LT. The train set and its nuclear architectural information extracted by U-net were used to train the MobileNet V2-based classifier (MobileNetV2_HCC_class). The classifier was then independently tested on the LT set and externally validated on the TCGA set (n = 302). The primary outcome was recurrence free survival (RFS).
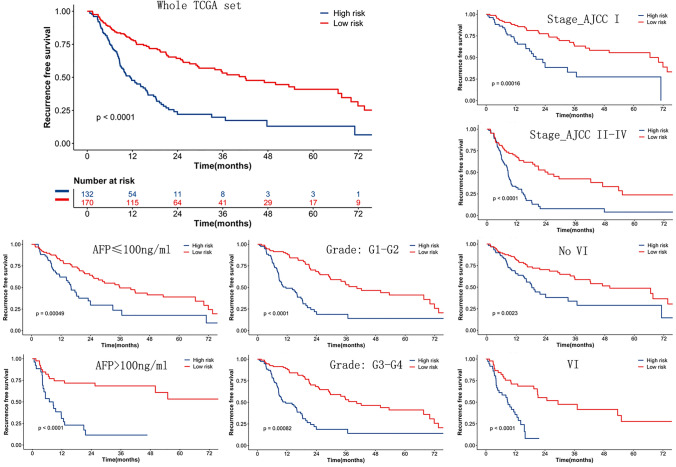
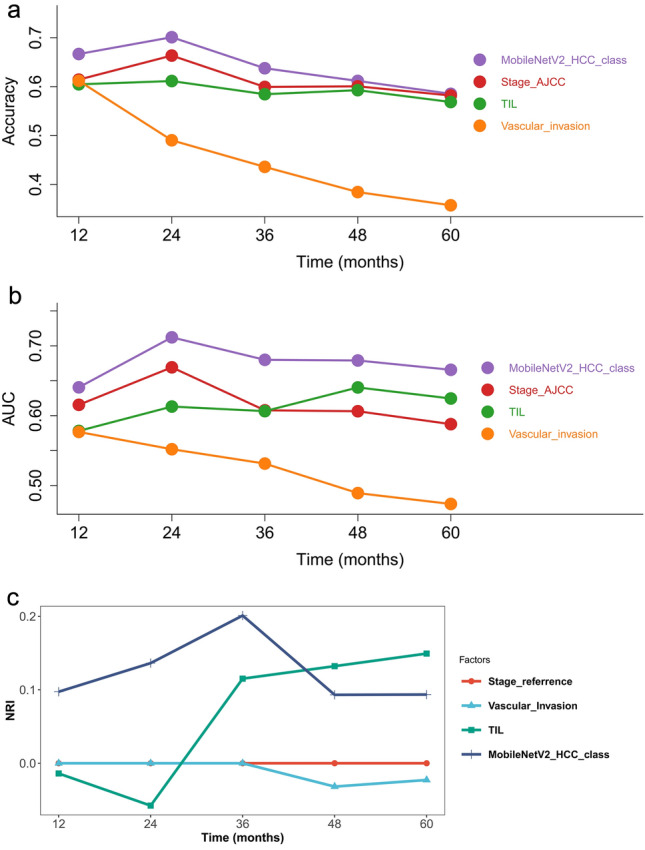
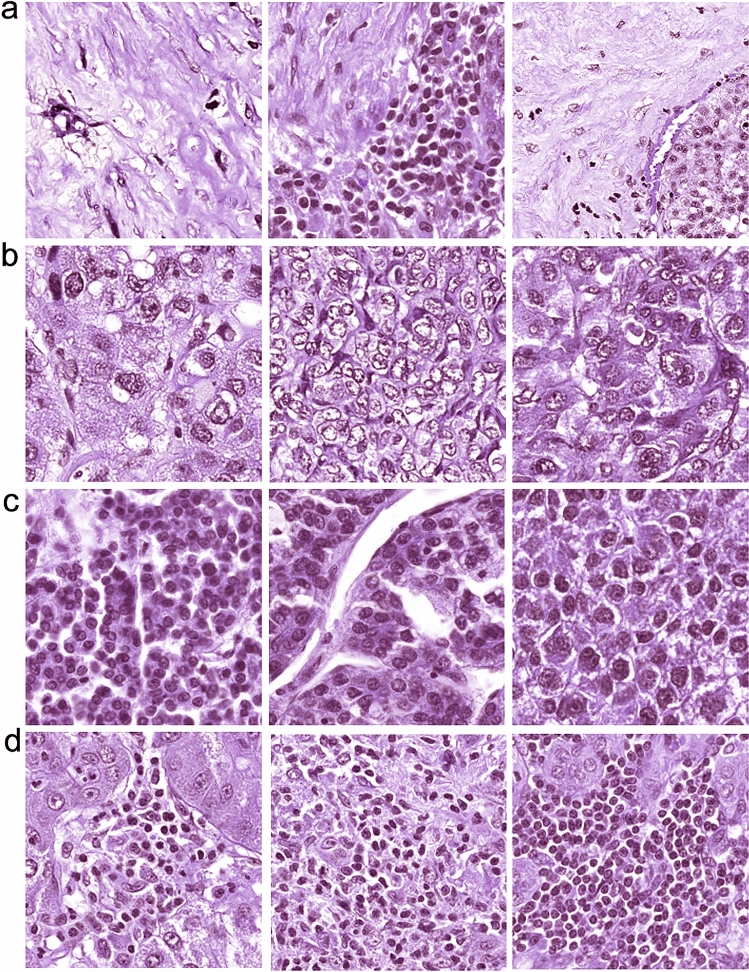
Results: The MobileNetV2_HCC_class was a strong predictor of RFS in both LT set and TCGA set. The classifier provided a hazard ratio of 3.44 (95% CI 2.01-5.87, p < 0.001) for high risk versus low risk in the LT set, and 2.55 (95% CI 1.64-3.99, p < 0.001) when known prognostic factors, remarkable in univariable analyses on the same cohort, were adjusted. The MobileNetV2_HCC_class maintained a relatively higher discriminatory power [time-dependent accuracy and area under curve (AUC)] than other factors after LT or resection in the independent validation set (LT and TCGA set). Net reclassification improvement (NRI) analysis indicated MobileNetV2_HCC_class exhibited better net benefits for the Stage_AJCC beyond other independent factors. A pathological review demonstrated that tumoral areas with the highest recurrence predictability featured the following features: the presence of stroma, a high degree of cytological atypia, nuclear hyperchromasia, and a lack of immune cell infiltration.
Conclusion: A prognostic classifier for clinical purposes had been proposed based on the use of deep learning on histological slides from HCC patients. This classifier assists in refining the prognostic prediction of HCC patients and identifies patients who have been benefited from more intensive management.
Keywords: Deep learning; HCC; LT; MobileNetV2; Prognosis.
© 2022. The Author(s).
Conflict of interest statement
Zhikun Liu, Yuanpeng Liu, Wenhui Zhang, Yuan Hong, Jinwen Meng, Jianguo Wang, Shusen Zheng and Xiao Xu have nothing to disclose.
Figures


References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
