

Importance of genetic testing in unexplained cardiac arrest
- PMID: 35352813
- PMCID: PMC9392649
- DOI: 10.1093/eurheartj/ehac145
Importance of genetic testing in unexplained cardiac arrest
Abstract
Aims: Genetic testing is recommended in specific inherited heart diseases but its role remains unclear and it is not currently recommended in unexplained cardiac arrest (UCA). We sought to assess the yield and clinical utility of genetic testing in UCA using whole-exome sequencing (WES).
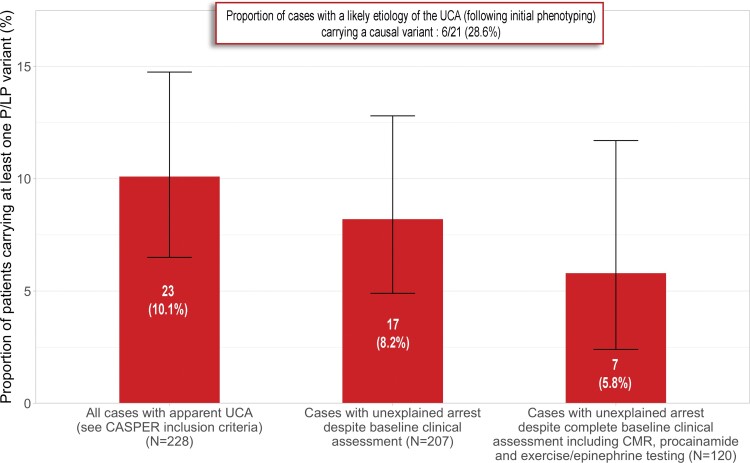
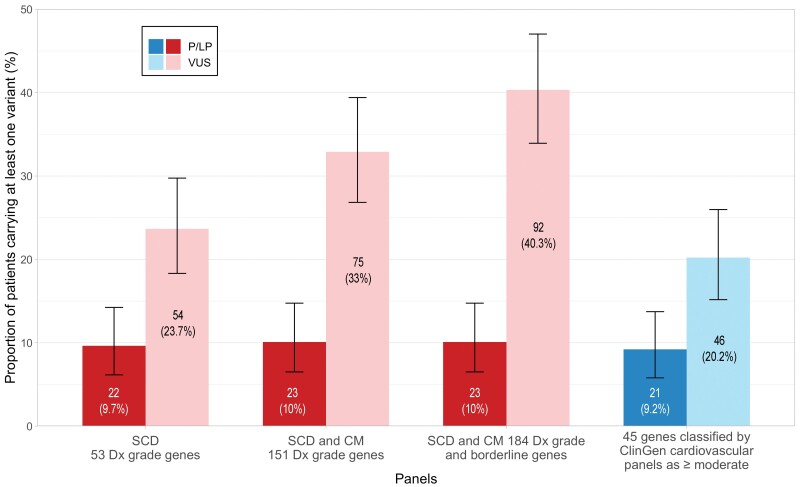
Methods and results: Survivors of UCA requiring external defibrillation were included from the Cardiac Arrest Survivor with Preserved Ejection fraction Registry. Whole-exome sequencing was performed, followed by assessment of rare variants in previously reported cardiovascular disease genes. A total of 228 UCA survivors (mean age at arrest 39 ± 13 years) were included. The majority were males (66%) and of European ancestry (81%). Following advanced clinical testing at baseline, the likely aetiology of cardiac arrest was determined in 21/228 (9%) cases. Whole-exome sequencing identified a pathogenic or likely pathogenic (P/LP) variant in 23/228 (10%) of UCA survivors overall, increasing the proportion of 'explained' cases from 9% only following phenotyping to 18% when combining phenotyping with WES. Notably, 13 (57%) of the 23 P/LP variants identified were located in genes associated with cardiomyopathy, in the absence of a diagnosis of cardiomyopathy at the time of arrest.
Conclusions: Genetic testing identifies a disease-causing variant in 10% of apparent UCA survivors. The majority of disease-causing variants was located in cardiomyopathy-associated genes, highlighting the arrhythmogenic potential of such variants in the absence of an overt cardiomyopathy diagnosis. The present study supports the use of genetic testing including assessment of arrhythmia and cardiomyopathy genes in survivors of UCA.
Keywords: Arrhythmia; Cardiac arrest; Cardiomyopathy; Cardiovascular genetics; Genetic testing; Ventricular fibrillation.
© The Author(s) 2022. Published by Oxford University Press on behalf of European Society of Cardiology.
Conflict of interest statement
Conflict of interest: The authors declare that there is no conflict of interest relevant to this study.
Figures


Comment in
-
Explaining the unexplained: applying genetic testing after cardiac arrest and sudden death.Eur Heart J. 2022 Aug 21;43(32):3082-3084. doi: 10.1093/eurheartj/ehac172. Eur Heart J. 2022. PMID: 35380654 No abstract available.
References
-
- Priori SG, Blomström-Lundqvist C, Mazzanti A, Blom N, Borggrefe M, Camm J, et al. 2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: The Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC). Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC). Eur Heart J 2015;36:2793–2867. 10.1093/eurheartj/ehv316. - DOI - PubMed
-
- Krahn AD, Healey JS, Chauhan V, Birnie DH, Simpson CS, Champagne J, et al. Systematic assessment of patients with unexplained cardiac arrest: Cardiac Arrest Survivors with Preserved Ejection Fraction Registry (CASPER). Circulation 2009;120:278–285. - PubMed
-
- Priori SG, Wilde AA, Horie M, Cho Y, Behr ER, Berul C, et al. Executive summary: HRS/EHRA/APHRS expert consensus statement on the diagnosis and management of patients with inherited primary arrhythmia syndromes. Europace 2013;15:1389–1406. - PubMed
-
- Ackerman MJ, Priori SG, Willems S, Berul C, Brugada R, Calkins H, et al. HRS/EHRA expert consensus statement on the state of genetic testing for the channelopathies and cardiomyopathies this document was developed as a partnership between the Heart Rhythm Society (HRS) and the European Heart Rhythm Association (EHRA). Heart Rhythm 2011;8:1308–1339. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
