

Assessment of Artificial Intelligence in Echocardiography Diagnostics in Differentiating Takotsubo Syndrome From Myocardial Infarction
- PMID: 35353118
- PMCID: PMC8968683
- DOI: 10.1001/jamacardio.2022.0183
Assessment of Artificial Intelligence in Echocardiography Diagnostics in Differentiating Takotsubo Syndrome From Myocardial Infarction
Abstract
Importance: Machine learning algorithms enable the automatic classification of cardiovascular diseases based on raw cardiac ultrasound imaging data. However, the utility of machine learning in distinguishing between takotsubo syndrome (TTS) and acute myocardial infarction (AMI) has not been studied.
Objectives: To assess the utility of machine learning systems for automatic discrimination of TTS and AMI.
Design, settings, and participants: This cohort study included clinical data and transthoracic echocardiogram results of patients with AMI from the Zurich Acute Coronary Syndrome Registry and patients with TTS obtained from 7 cardiovascular centers in the International Takotsubo Registry. Data from the validation cohort were obtained from April 2011 to February 2017. Data from the training cohort were obtained from March 2017 to May 2019. Data were analyzed from September 2019 to June 2021.
Exposure: Transthoracic echocardiograms of 224 patients with TTS and 224 patients with AMI were analyzed.
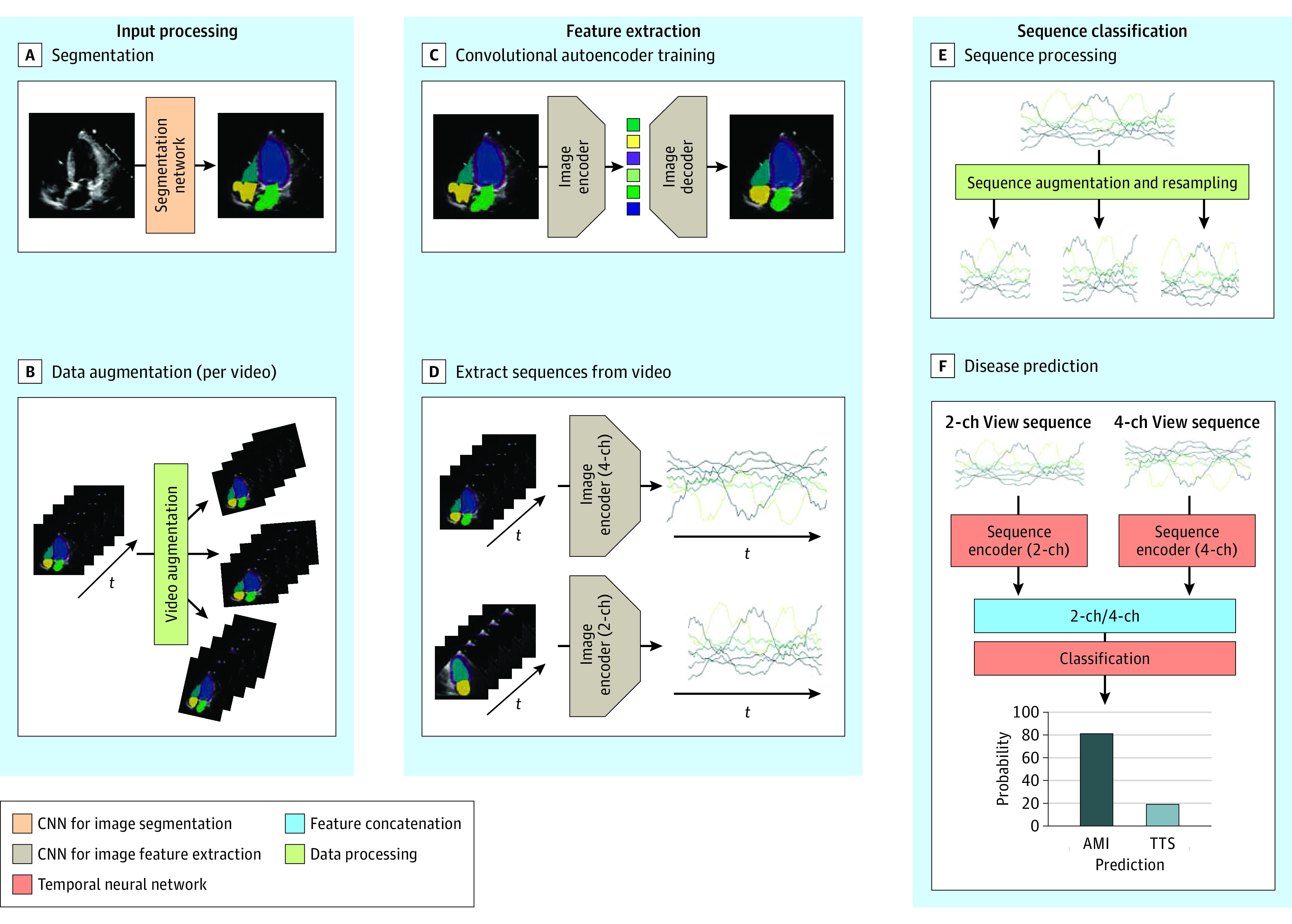
Main outcomes and measures: Area under the receiver operating characteristic curve (AUC), accuracy, sensitivity, and specificity of the machine learning system evaluated on an independent data set and 4 practicing cardiologists for comparison. Echocardiography videos of 228 patients were used in the development and training of a deep learning model. The performance of the automated echocardiogram video analysis method was evaluated on an independent data set consisting of 220 patients. Data were matched according to age, sex, and ST-segment elevation/non-ST-segment elevation (1 patient with AMI for each patient with TTS). Predictions were compared with echocardiographic-based interpretations from 4 practicing cardiologists in terms of sensitivity, specificity, and AUC calculated from confidence scores concerning their binary diagnosis.
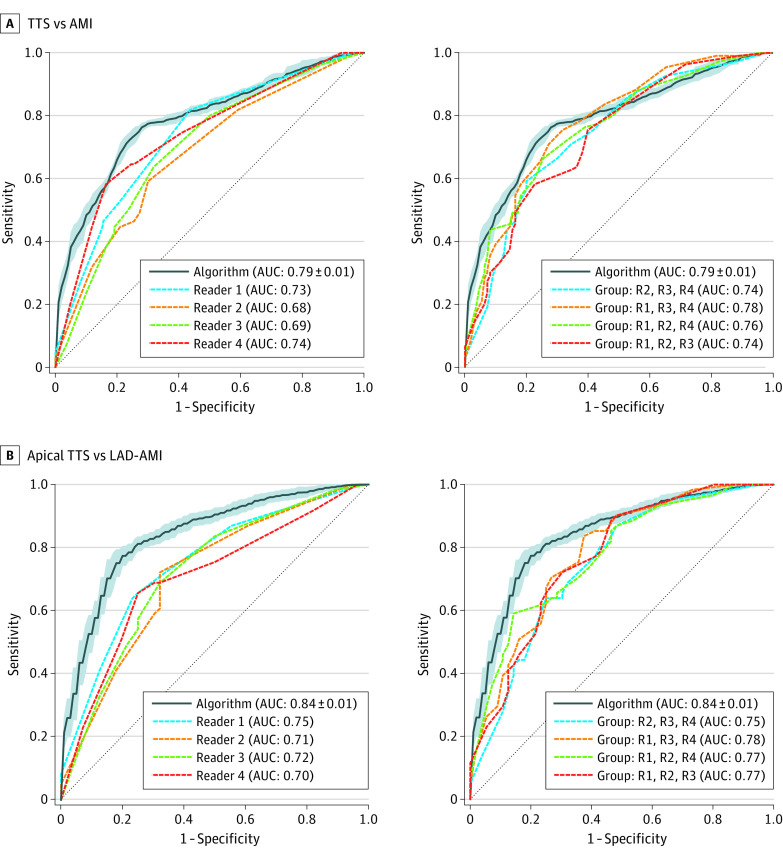
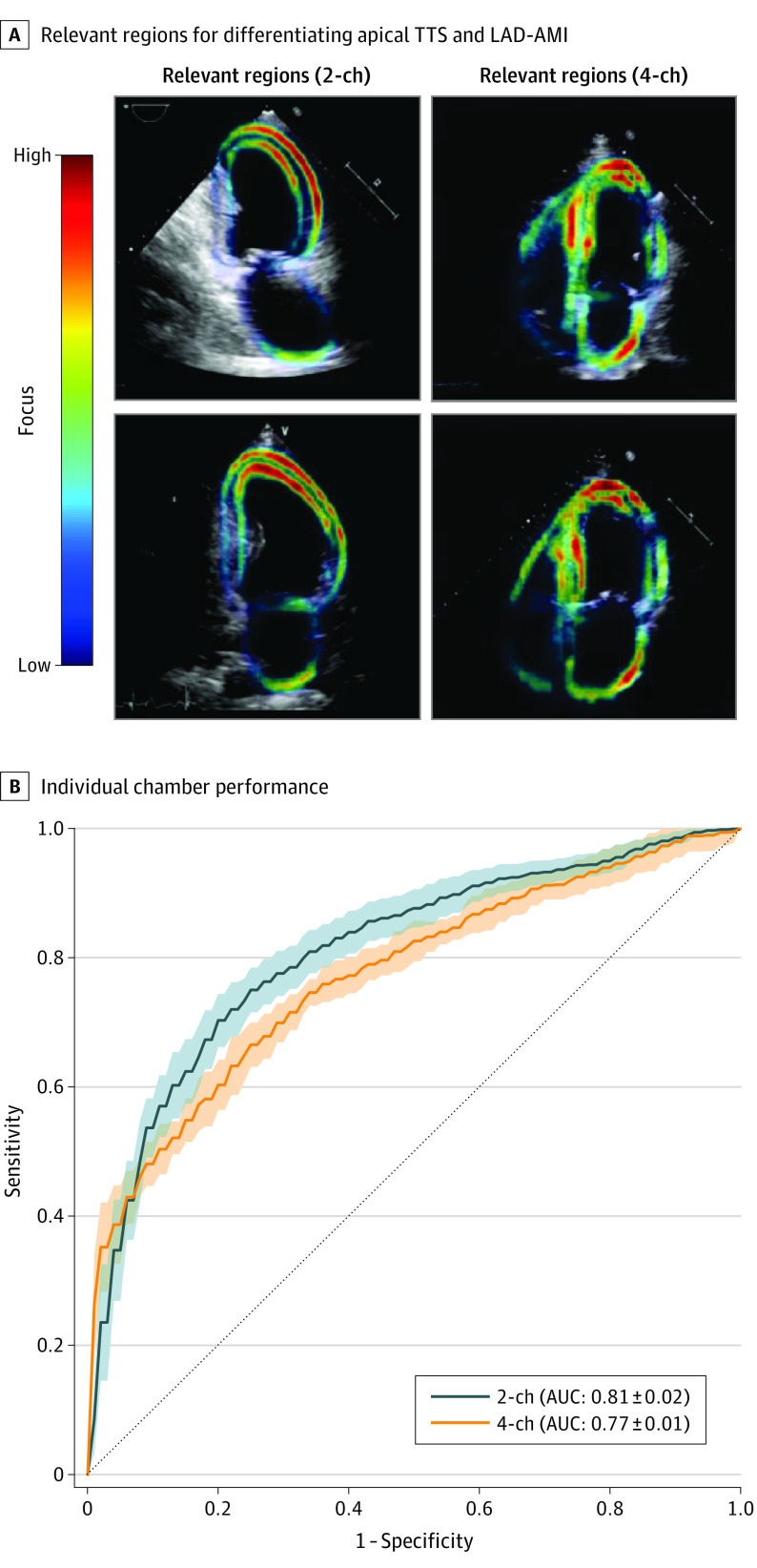
Results: In this cohort study, apical 2-chamber and 4-chamber echocardiographic views of 110 patients with TTS (mean [SD] age, 68.4 [12.1] years; 103 [90.4%] were female) and 110 patients with AMI (mean [SD] age, 69.1 [12.2] years; 103 [90.4%] were female) from an independent data set were evaluated. This approach achieved a mean (SD) AUC of 0.79 (0.01) with an overall accuracy of 74.8 (0.7%). In comparison, cardiologists achieved a mean (SD) AUC of 0.71 (0.03) and accuracy of 64.4 (3.5%) on the same data set. In a subanalysis based on 61 patients with apical TTS and 56 patients with AMI due to occlusion of the left anterior descending coronary artery, the model achieved a mean (SD) AUC score of 0.84 (0.01) and an accuracy of 78.6 (1.6%), outperforming the 4 practicing cardiologists (mean [SD] AUC, 0.72 [0.02]) and accuracy of 66.9 (2.8%).
Conclusions and relevance: In this cohort study, a real-time system for fully automated interpretation of echocardiogram videos was established and trained to differentiate TTS from AMI. While this system was more accurate than cardiologists in echocardiography-based disease classification, further studies are warranted for clinical application.
Conflict of interest statement
Figures
Comment in
-
Validating Deep Learning to Distinguish Takotsubo Syndrome From Acute Myocardial Infarction-Beware of Shortcuts, Human Supervision Required.JAMA Cardiol. 2022 May 1;7(5):477-479. doi: 10.1001/jamacardio.2022.0193. JAMA Cardiol. 2022. PMID: 35353132 No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
