

Analysis of Adverse Events and Intravenous Iron Infusion Formulations in Adults With and Without Prior Infusion Reactions
- PMID: 35353168
- PMCID: PMC8968468
- DOI: 10.1001/jamanetworkopen.2022.4488
Analysis of Adverse Events and Intravenous Iron Infusion Formulations in Adults With and Without Prior Infusion Reactions
Erratum in
-
Error in Byline.JAMA Netw Open. 2022 Jun 1;5(6):e2221567. doi: 10.1001/jamanetworkopen.2022.21567. JAMA Netw Open. 2022. PMID: 35731522 Free PMC article. No abstract available.
Abstract
Importance: Although iron deficiency is common, it remains unclear which iron repletion strategy is associated with the lowest rate of infusion-related adverse events, and how patients with history of infusion reaction should be managed.
Objective: To evaluate rates of infusion reactions among 4 commonly used intravenous iron repletion strategies and determine how readministration was managed in patients with history of reaction.
Design, setting, and participants: This cohort study included all patients receiving intravenous iron infusion from January 1, 2015, to September 7, 2021, at 6 centers in Portland, Oregon. Participants included a total of 12 237 patients with iron deficiency, not restricted by etiology. Statistical analysis was performed from September to October 2021.
Exposures: Type of intravenous iron formulation and concurrent administration of diphenhydramine, epinephrine, famotidine, and/or hydrocortisone, used as surrogate maker of infusion reaction.
Main outcomes and measures: Incidence of adverse events, including severe events requiring epinephrine, stratified by type of iron formulation, and in patients who received premedication or with history of infusion-related reaction receiving subsequent doses.
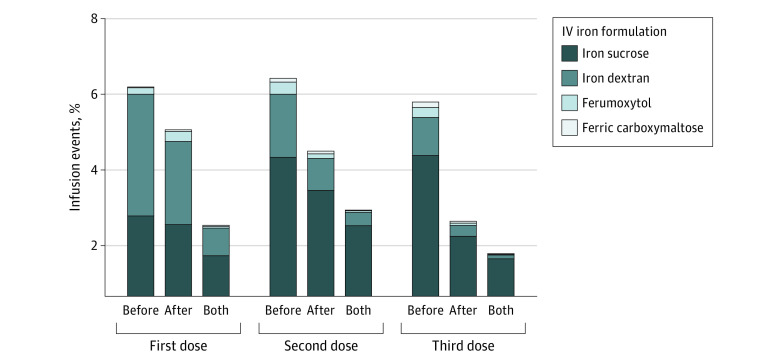
Results: Among 35 737 unique iron infusions (12 237 patients [9480 (77.5%) women; 717 (5.9%) Black; 10 250 (83.7%) White; mean (SD) age of 51 (20) years]), comprising 22 309 iron sucrose doses, 9067 iron dextran total doses (1771 preceded by test dose, 56 test doses alone), 3147 ferumoxytol doses, and 1214 ferric carboxymaltose doses, incidence of adverse events was 3.9% (n = 1389; 95% CI, 3.7%-4.1%). Rate of infusion events differed among iron formulations: 4.3% (n = 970; 95% CI, 4.1%-4.6%) iron sucrose, 3.8% (n = 345, 95% CI: 3.4%-4.2%) iron dextran (test and full doses or test dose alone), 1.8% (n = 57; 95% CI, 1.4%-2.3%) ferumoxytol, and 1.4% (n = 17, 95% CI, 0.8%-2.3%) ferric carboxymaltose (P < .001). Severe adverse events were exceedingly rare with only 2 documented epinephrine administrations, both associated with iron dextran. Incidence of adverse events among those who received premedication was 23-fold higher compared with those who did not (38.6% vs 1.7%, χ21 = 7324.8; P < .001). Among 873 patients with history of infusion reaction who underwent readministration, the majority received the same formulation, which was associated with significantly higher reaction rate particularly if premedication was administered (68% [95% CI, 64%-72%] vs 32% [95% CI, 26%-41%], respectively), compared with those who received an alternate formulation (21% [95% CI, 11%-35%] vs 5% [95% CI, 2%-12%], respectively) (P < .001).
Conclusions and relevance: These data, and the preponderance of published evidence, suggest that intravenous iron is generally well tolerated with exceedingly low risk of severe reaction, use of premedication and test doses are unnecessary, and that optimal prevention and management of infusion-related reactions warrant further study.
Conflict of interest statement
Figures
Comment in
-
Unanswered questions from the IRONMAN trial.Lancet. 2023 May 6;401(10387):1494-1495. doi: 10.1016/S0140-6736(23)00447-6. Lancet. 2023. PMID: 37149299 No abstract available.
-
Unanswered questions from the IRONMAN trial.Lancet. 2023 May 6;401(10387):1495. doi: 10.1016/S0140-6736(23)00449-X. Lancet. 2023. PMID: 37149300 No abstract available.
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
