

Effectiveness of Mechanical Chest Compression Devices over Manual Cardiopulmonary Resuscitation: A Systematic Review with Meta-analysis and Trial Sequential Analysis
- PMID: 35353993
- PMCID: PMC8328162
- DOI: 10.5811/westjem.2021.3.50932
Effectiveness of Mechanical Chest Compression Devices over Manual Cardiopulmonary Resuscitation: A Systematic Review with Meta-analysis and Trial Sequential Analysis
Abstract
Introduction: Our goal was to systematically review contemporary literature comparing the relative effectiveness of two mechanical compression devices (LUCAS and AutoPulse) to manual compression for achieving return of spontaneous circulation (ROSC) in patients undergoing cardiopulmonary resuscitation (CPR) after an out-of-hospital cardiac arrest (OHCA).
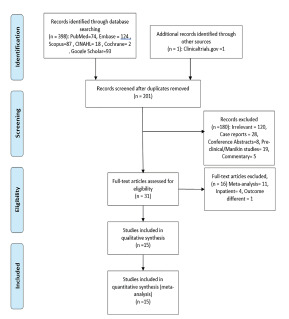
Methods: We searched medical databases systematically for randomized controlled trials (RCT) and observational studies published between January 1, 2000-October 1, 2020 that compared mechanical chest compression (using any device) with manual chest compression following OHCA. We only included studies in the English language that reported ROSC outcomes in adult patients in non-trauma settings to conduct random-effects metanalysis and trial sequence analysis (TSA). Multivariate meta-regression was performed using preselected covariates to account for heterogeneity. We assessed for risk of biases in randomization, allocation sequence concealment, blinding, incomplete outcome data, and selective outcome reporting.
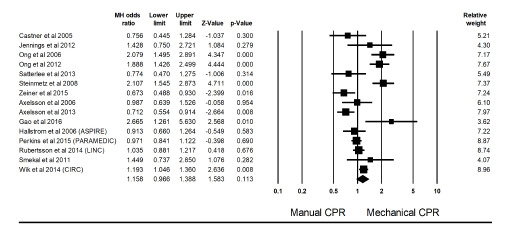
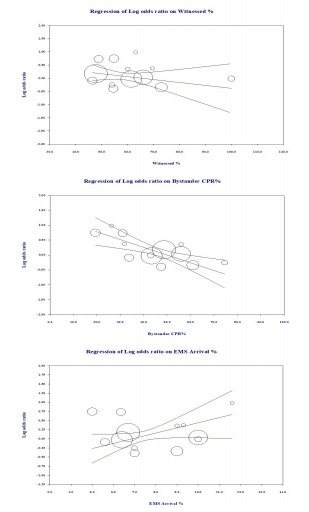
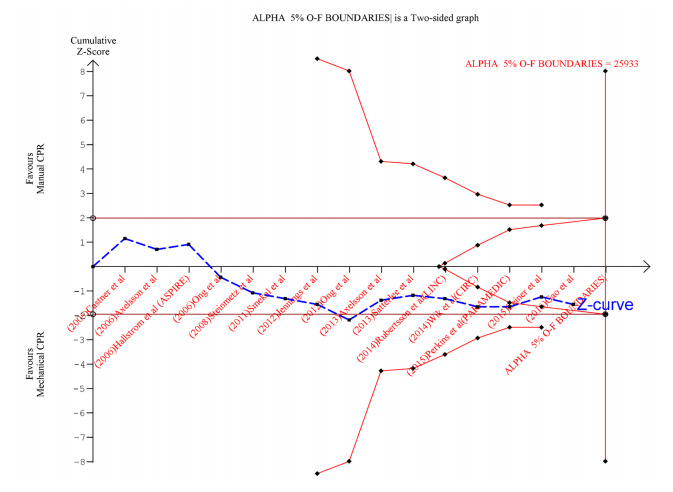
Results: A total of 15 studies (n = 18474), including six RCTs, two cluster RCTs, five retrospective case-control, and two phased prospective cohort studies, were pooled for analysis. The pooled estimates' summary effect did not indicate a significant difference (Mantel-Haenszel odds ratio = 1.16, 95% confidence interval, 0.97 to 1.39, P = 0.11, I2 = 0.83) between mechanical and manual compressions during CPR for ROSC. The TSA showed firm evidence supporting the lack of improvement in ROSC using mechanical compression devices. The Z-curves successfully crossed the TSA futility boundary for ROSC, indicating sufficient evidence to draw firm conclusions regarding these outcomes. Multivariate meta-regression demonstrated that 100% of the between-study variation could be explained by differences in average age, the proportion of females, cardiac arrests with shockable rhythms, witnessed cardiac arrest, bystander CPR, and the average time for emergency medical services (EMS) arrival in the study samples, with the latter three attaining statistical significance.
Conclusion: Mechanical compression devices for resuscitation in cardiac arrests are not associated with improved rates of ROSC. Their use may be more beneficial in non-ideal situations such as lack of bystander CPR, unwitnessed arrest, and delayed EMS response times. Studies done to date have enough power to render further studies on this comparison futile.
Conflict of interest statement
Figures
References
-
- Hazinski MF, Nolan JP, Aickin R, et al. Part 1: Executive Summary: 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation. 2015;132(16_suppl_1):S2–S39. - PubMed
-
- Ottawa Hospital Research Institute. [Accessed November 8, 2020]. Available at: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials