

Bevacizumab versus PARP-inhibitors in women with newly diagnosed ovarian cancer: a network meta-analysis
- PMID: 35354431
- PMCID: PMC8969379
- DOI: 10.1186/s12885-022-09455-x
Bevacizumab versus PARP-inhibitors in women with newly diagnosed ovarian cancer: a network meta-analysis
Abstract
Background: In women with newly diagnosed ovarian cancer, bevacizumab and poly (ADP-ribose) polymerase inhibitors (PARPi) exhibit improved progression-free survival (PFS) when administered concurrent with chemotherapy and/or maintenance therapy, but no study has directly compared their effects. Therefore, this study aimed to compare the efficacy and safety of bevacizumab and PARPi in women with newly diagnosed ovarian cancer using a network meta-analysis.
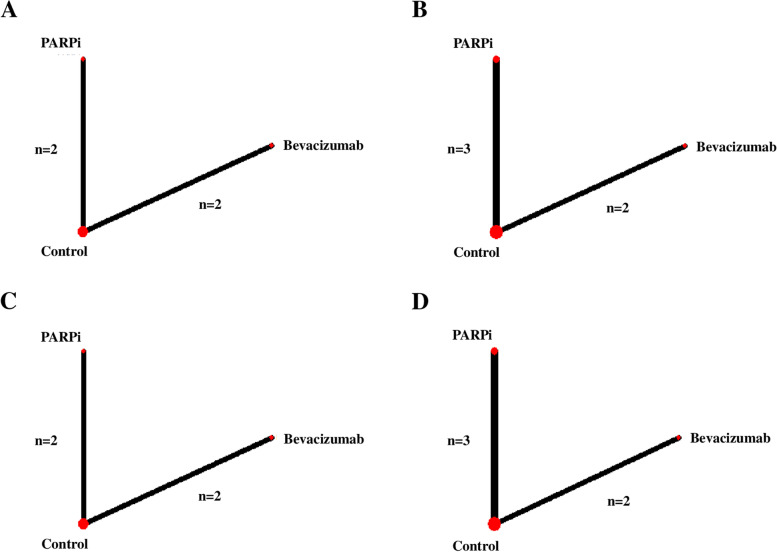
Methods: PubMed, Medline, and Embase databases were searched, and five randomized trials assessing PFS in women with newly diagnosed ovarian cancer treated with either bevacizumab, PARPi, or placebo or no additional agent (controls) were identified. PFS was compared in the overall population with ovarian cancer, women with a BRCA1/2 mutation (BRCAm) and women with homologous-recombination deficiency (HRD). Adverse events (grade ≥ 3) were compared in all populations of the included studies.
Results: PARPi improved PFS significantly more than bevacizumab in women with a BRCAm (HR 0.47; 95% CI 0.36-0.60) and with HRD (HR 0.66; 95% CI 0.50-0.87). However, in the overall population with ovarian cancer, no significant difference in PFS was observed between women treated with PARPi and those treated with bevacizumab. PARPi exhibited the highest surface under the cumulative ranking probabilities value as the most effective treatment for PFS (PARPi vs. bevacizumab: 98% vs. 52% in the overall population with ovarian cancer; 100% vs. 50% in women with BRCAm; 100% vs. 50% in women with HRD). For adverse events, the risk of all treatments was similar. However, PARPi had a higher adverse risk than the control group (relative risk 2.14; 95% CI 1.40-3.26).
Conclusions: In women with newly diagnosed ovarian cancer, PARPi might be more effective in terms of PFS compared to bevacizumab. The risk of serious adverse events was similar for PARPi and bevacizumab.
Keywords: Adverse events; BRCA mutation; Bevacizumab; Homologous recombination deficiency; Ovarian cancer; Poly(ADP-ribose) polymerase inhibitors; Progression-free survival.
© 2022. The Author(s).
Conflict of interest statement
The authors have no conflict of interest or financial ties to disclose.
Figures


References
-
- Aghajanian C, Blank SV, Goff BA, Judson PL, Teneriello MG, Husain A, et al. OCEANS: A randomized, double-blind, placebo-controlled phase III trial of chemotherapy with or without bevacizumab in patients with platinum-sensitive recurrent epithelial ovarian, primary peritoneal, or fallopian tube Cancer. J Clin Oncol. 2012;30:2039–2045. doi: 10.1200/JCO.2012.42.0505. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
