

Peripheral primitive neuroectodermal tumor: a case report
- PMID: 35354472
- PMCID: PMC8969283
- DOI: 10.1186/s13256-022-03354-2
Peripheral primitive neuroectodermal tumor: a case report
Abstract
Background: Primitive neuroectodermal tumors are extremely rare and highly aggressive malignant small round cell tumors that arise from the primitive nerve cells of the nervous system or outside it. These tumors share similar histology, immunohistologic characteristics, and cytogenetics with Ewing's sarcoma. Peripheral primitive neuroectodermal tumors of the chest wall are rare malignant tumors seen in children and young adults.
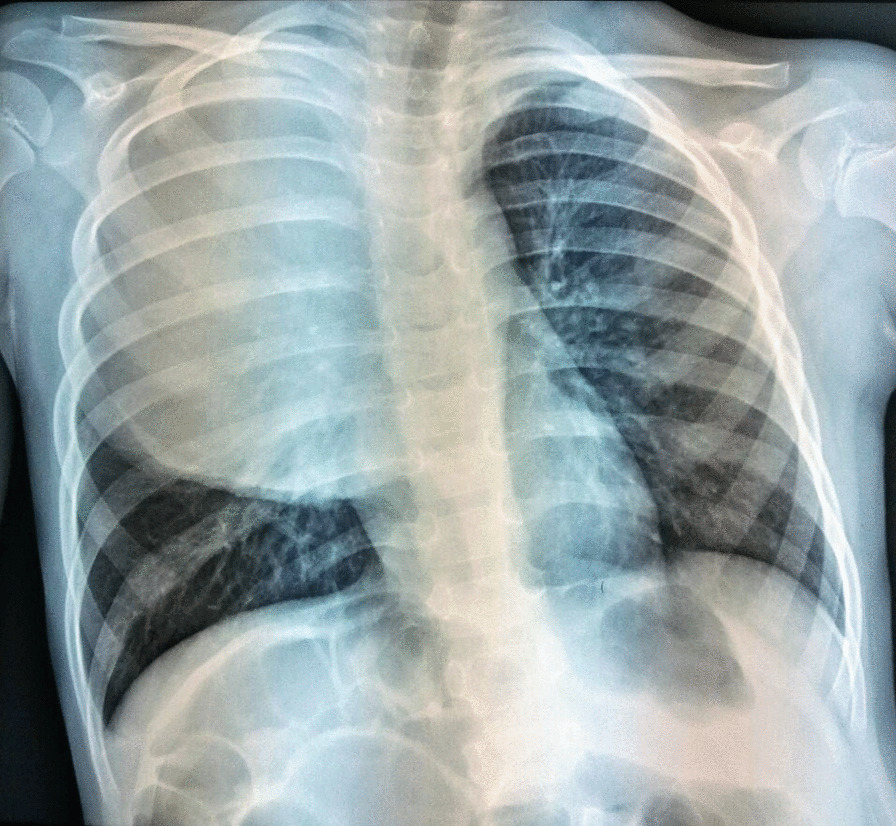
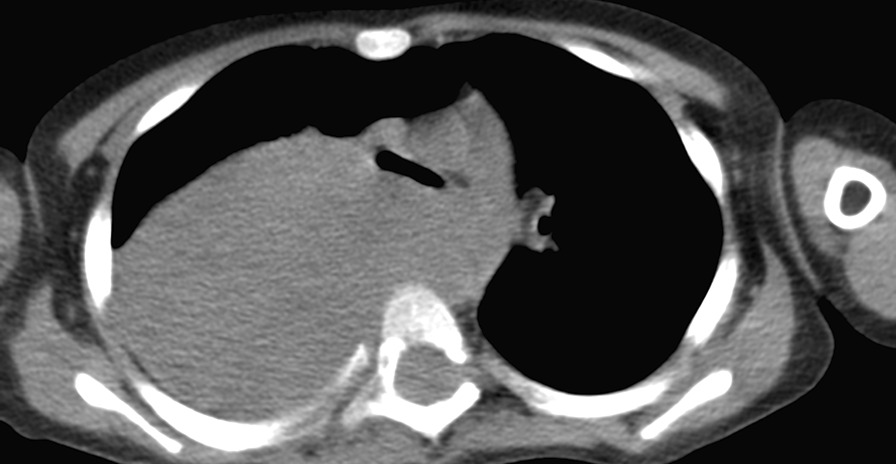
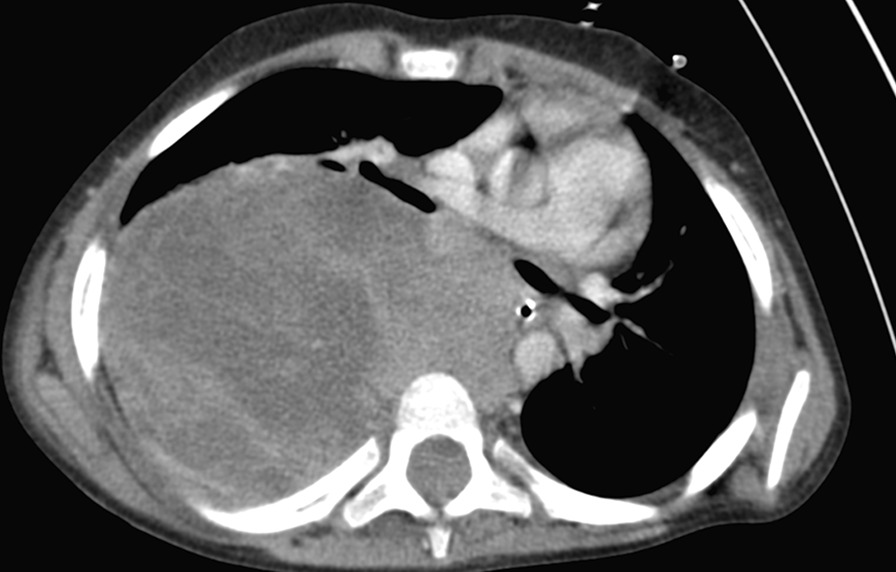
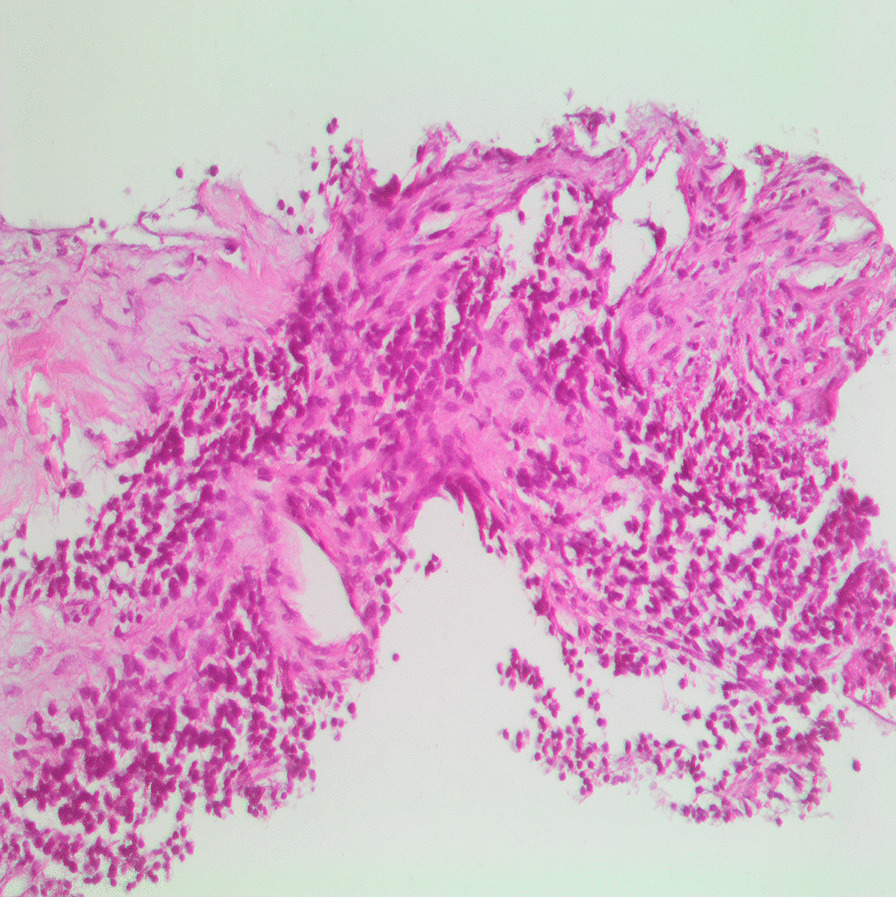
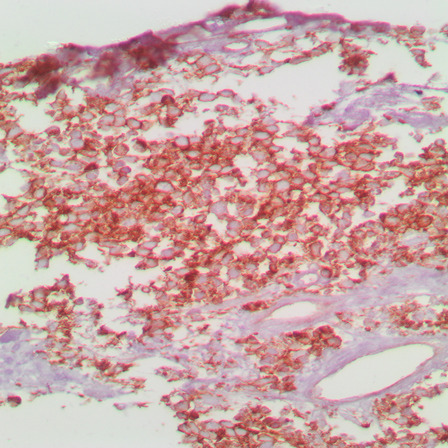
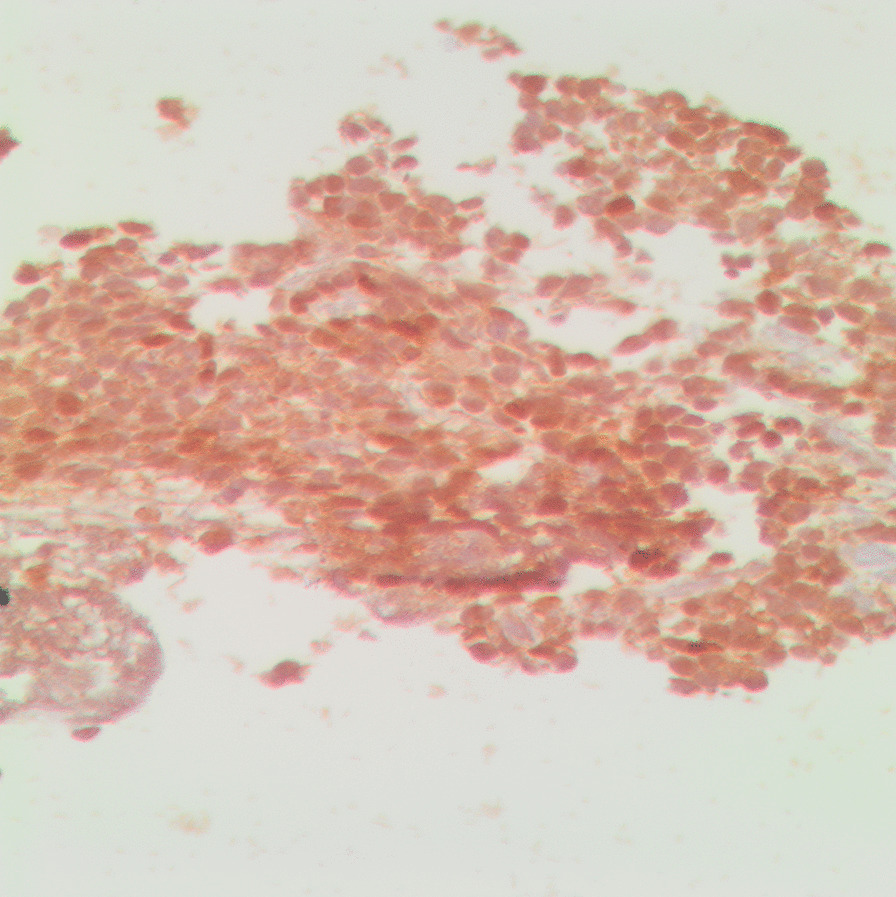
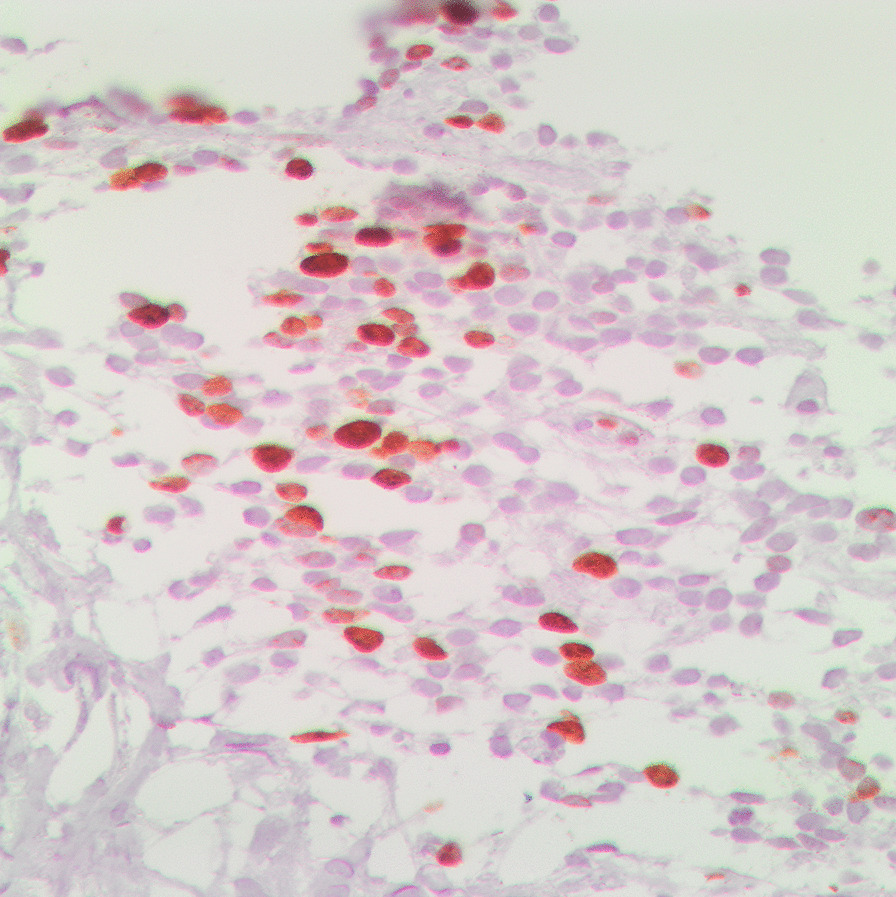
Case presentation: We report a rare case of peripheral primitive neuroectodermal tumor in a 4-year-old Albanian girl with a mediastinal tumor and an unusual clinical presentation. She was initially treated for acute polyradiculoneuritis (Guillain-Barré syndrome) owing to pain, weakness in the lower limbs, and walking difficulty, as well as severe irritability. During the second week of treatment, the child began to experience dry cough, chest discomfort, and worsening dyspnea. Chest radiography, chest computed tomography, and contrast-enhanced computed tomography demonstrated a large mass in the right hemithorax that was derived from the posterior mediastinum with expansive growth in all directions and that shifted the mediastinal structures in the anterolateral left direction. Consequently, histopathology and immunohistochemical examination of the markers S-100, CD99, and Ki-67 showed that the tumor cells stained positively for S-100 and CD99. The proliferative index measured by Ki-67 was approximately 20%, which suggested primitive neuroectodermal tumor.
Conclusions: Even though other diseases, including leukemia, lymphoma, and neuroblastoma, may be accompanied by musculoskeletal manifestations in children, other solid tumors, such as peripheral primitive neuroectodermal tumors, should be considered in the differential diagnosis in any child presenting with musculoskeletal symptoms.
Keywords: Children; Mediastinal tumor; Musculoskeletal manifestations; Primitive neuroectodermal tumor.
© 2022. The Author(s).
Conflict of interest statement
There are no competing interests to disclose.
Figures
References
-
- Qian Xu Q. Askin tumor: four case reports and a review of the literature. 2011. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3266582/ [Accessed 28 May 2019]. - PMC - PubMed
-
- Mangham D. World Health Organisation classification of tumours: pathology and genetics of tumours of soft tissue and bone. J Bone Jt Surg Br. 2004;86(33):466–466. doi: 10.1302/0301-620X.86B3.0860466b. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
