

Evaluation of the learning curve for conformal sphincter preservation operation in the treatment of ultralow rectal cancer
- PMID: 35354489
- PMCID: PMC8966240
- DOI: 10.1186/s12957-022-02541-1
Evaluation of the learning curve for conformal sphincter preservation operation in the treatment of ultralow rectal cancer
Abstract
Background: To investigate the learning curve of conformal sphincter preservation operation (CSPO) in the treatment of ultralow rectal cancer and to further explore the influencing factors of operation time.
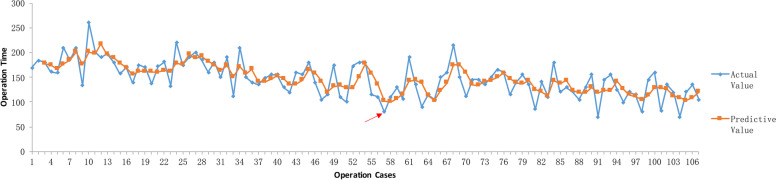
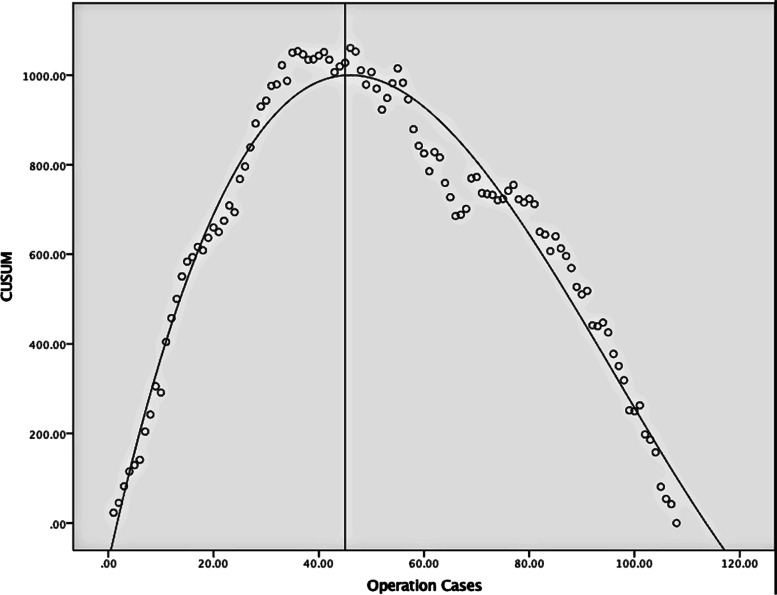
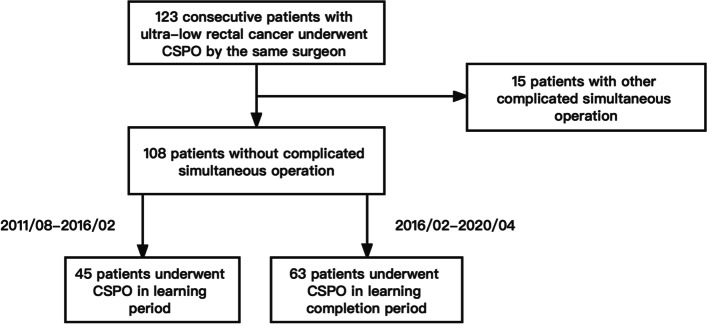
Methods: From August 2011 to April 2020, 108 consecutive patients with ultralow rectal cancer underwent CSPO by the same surgeon in the Department of Colorectal Surgery of Changhai Hospital. The moving average and cumulative sum control chart (CUSUM) curve were used to analyze the learning curve. The preoperative clinical baseline data, postoperative pathological data, postoperative complications, and survival data were compared before and after the completion of learning curve. The influencing factors of CSPO operation time were analyzed by univariate and multivariate analysis.
Results: According to the results of moving average and CUSUM method, CSPO learning curve was divided into learning period (1-45 cases) and learning completion period (46-108 cases). There was no significant difference in preoperative clinical baseline data, postoperative pathological data, postoperative complications, and survival data between the two stages. Compared with the learning period, the operation time (P < 0.05), blood loss (P < 0.05), postoperative flatus and defecation time (P < 0.05), liquid diet time (P < 0.05), and postoperative hospital stay (P < 0.05) in the learning completion period were significantly reduced, and the difference was statistically significant. Univariate and multivariate analysis showed that distance of tumor from anal verge (≥ 4cm vs. < 4cm, P = 0.039) and T stage (T3 vs. T1-2, P = 0.022) was independent risk factors for prolonging the operation time of CSPO.
Conclusions: For surgeons with laparoscopic surgery experience, about 45 cases of CSPO are needed to cross the learning curve. At the initial stage of CSPO, beginners are recommended to select patients with ultralow rectal cancer whose distance of tumor from anal verge is less than 4 cm and tumor stage is less than T3 for practice, which can enable beginners to reduce the operation time, accumulate experience, build self-confidence, and shorten the learning curve on the premise of safety.
Keywords: Conformal sphincter preservation operation; Learning curve; Operation time; Ultralow rectal cancer.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
