

Association of computed tomography screening with lung cancer stage shift and survival in the United States: quasi-experimental study
- PMID: 35354556
- PMCID: PMC8965744
- DOI: 10.1136/bmj-2021-069008
Association of computed tomography screening with lung cancer stage shift and survival in the United States: quasi-experimental study
Abstract
Objective: To determine the effect of the introduction of low dose computed tomography screening in 2013 on lung cancer stage shift, survival, and disparities in the stage of lung cancer diagnosed in the United States.
Design: Quasi-experimental study using Joinpoint modeling, multivariable ordinal logistic regression, and multivariable Cox proportional hazards modeling.
Setting: US National Cancer Database and Surveillance Epidemiology End Results program database.
Participants: Patients aged 45-80 years diagnosed as having non-small cell lung cancer (NSCLC) between 1 January 2010 and 31 December 2018.
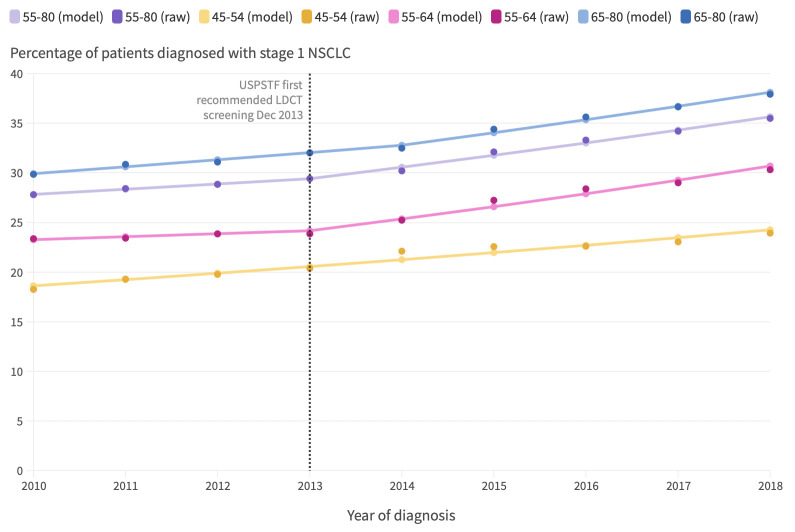
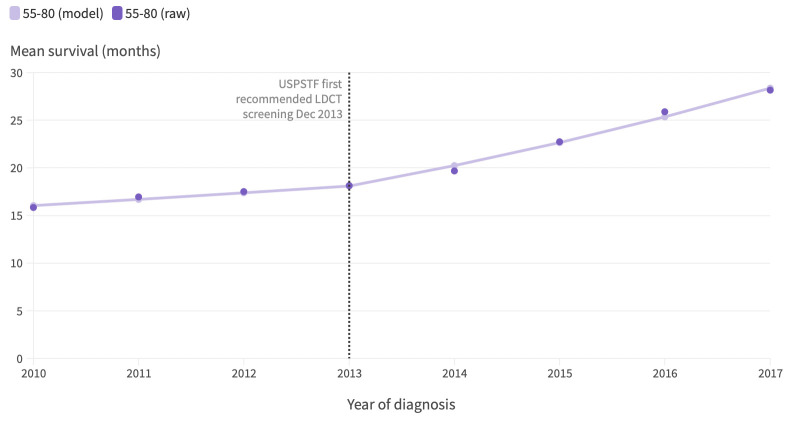
Main outcome measures: Annual per cent change in percentage of stage I NSCLC diagnosed among patients aged 45-54 (ineligible for screening) and 55-80 (potentially eligible for screening), median all cause survival, and incidence of NSCLC; multivariable adjusted odds ratios for year-to-year changes in likelihood of having earlier stages of disease at diagnosis and multivariable adjusted hazard ratios for changes in hazard of death before versus after introduction of screening.
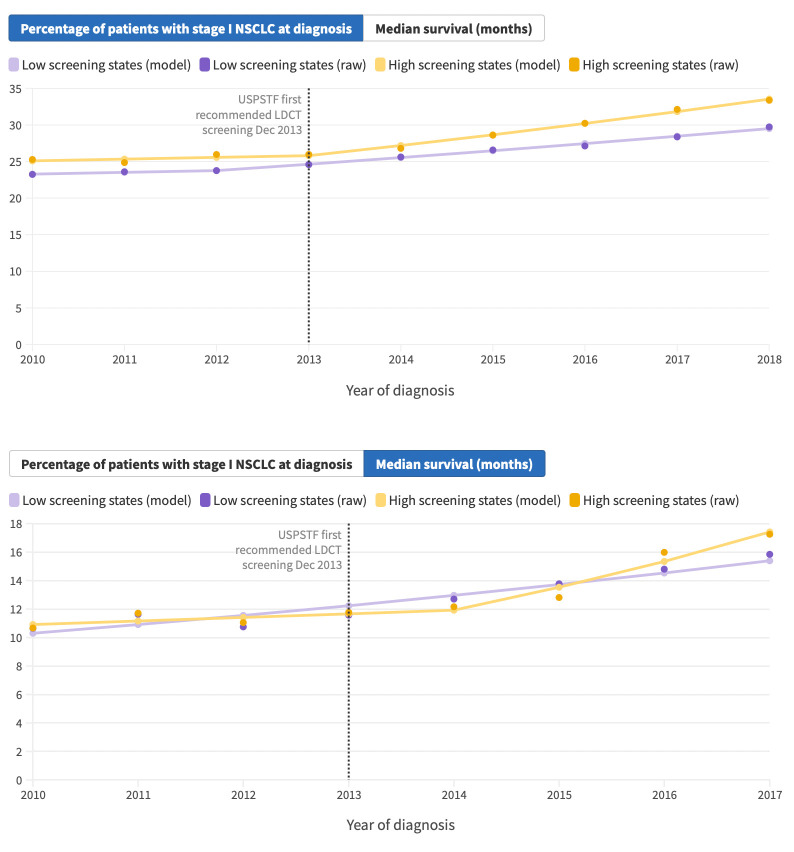
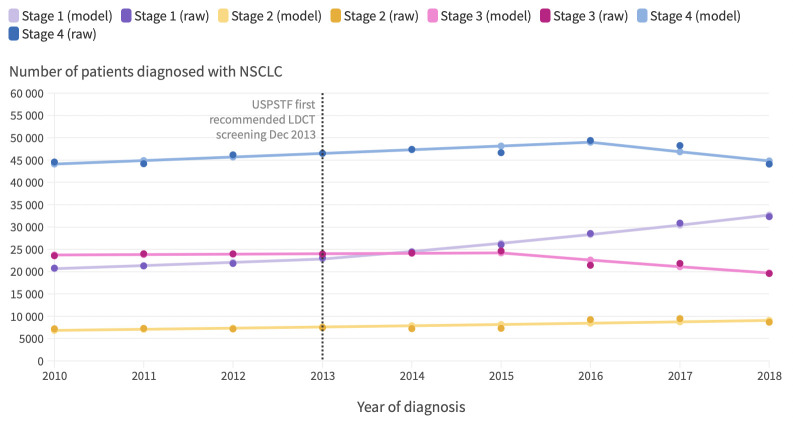
Results: The percentage of stage I NSCLC diagnosed among patients aged 55-80 did not significantly increase from 2010 to 2013 (from 27.8% to 29.4%) and then increased at 3.9% (95% confidence interval 3.0% to 4.8%) per year from 2014 to 2018 (from 30.2% to 35.5%). In multivariable adjusted analysis, the increase in the odds per year of a patient having one lung cancer stage lower at diagnosis during the time period from 2014 to 2018 was 6.2% (multivariable adjusted odds ratio 1.062, 95% confidence interval 1.048 to 1.077; P<0.001) higher than the increase in the odds per year from 2010 to 2013. Similarly, the median all cause survival of patients aged 55-80 did not significantly increase from 2010 to 2013 (from 15.8 to 18.1 months), and then increased at 11.9% (8.9% to 15.0%) per year from 2014 to 2018 (from 19.7 to 28.2 months). In multivariable adjusted analysis, the hazard of death decreased significantly faster after 2014 compared with before 2014 (P<0.001). By 2018, stage I NSCLC was the predominant diagnosis among non-Hispanic white people and people living in the highest income or best educated regions. Non-white people and those living in lower income or less educated regions remained more likely to have stage IV disease at diagnosis. Increases in the detection of early stage disease in the US from 2014 to 2018 led to an estimated 10 100 averted deaths.
Conclusions: A recent stage shift toward stage I NSCLC coincides with improved survival and the introduction of lung cancer screening. Non-white patients and those living in areas of greater deprivation had lower rates of stage I disease identified, highlighting the need for efforts to increase access to screening in the US.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/disclosure-of-interest/ and declare: no support from any organization for the submitted work; no financial relationships with any organizations that might have an interest in the submitted work in the previous three years; ALP, ALR, and CJY have leadership roles in the American Lung Cancer Screening Initiative.
Figures

Comment in
-
Screening high risk populations for lung cancer.BMJ. 2022 Mar 30;376:o666. doi: 10.1136/bmj.o666. BMJ. 2022. PMID: 35354585 No abstract available.
References
-
- US Preventive Services Task Force. Lung Cancer: Screening. 2021. https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/lung....
MeSH terms
LinkOut - more resources
Full Text Sources
Medical