

Mortality after acute kidney injury and acute interstitial nephritis in patients prescribed immune checkpoint inhibitor therapy
- PMID: 35354588
- PMCID: PMC8968986
- DOI: 10.1136/jitc-2021-004421
Mortality after acute kidney injury and acute interstitial nephritis in patients prescribed immune checkpoint inhibitor therapy
Abstract
Background: In patients receiving immune checkpoint inhibitor (ICI) therapy, acute kidney injury (AKI) is common, and can occur either from kidney injury unrelated to ICI use or from immune activation resulting in acute interstitial nephritis (AIN). In this study, we test the hypothesis that occurrence of AIN indicates a favorable treatment response to ICI therapy and therefore among patients who develop AKI while on ICI therapy, those with AIN will demonstrate greater survival compared with others with AKI.
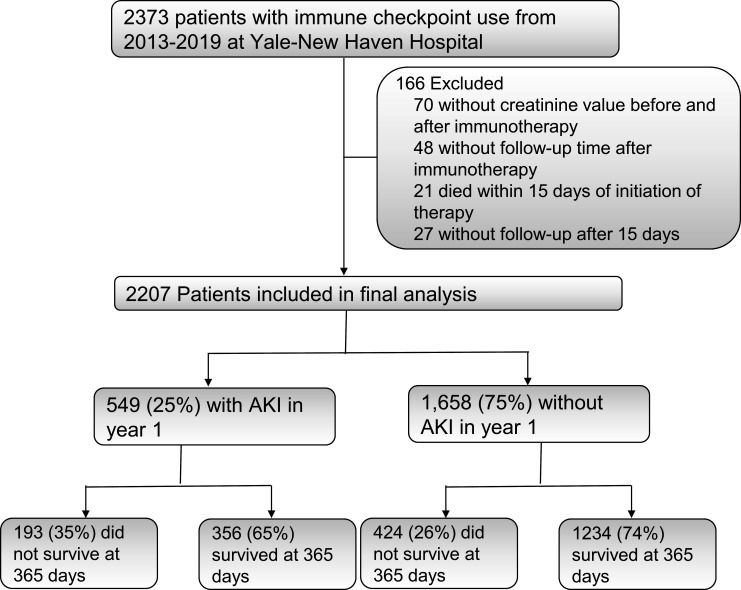
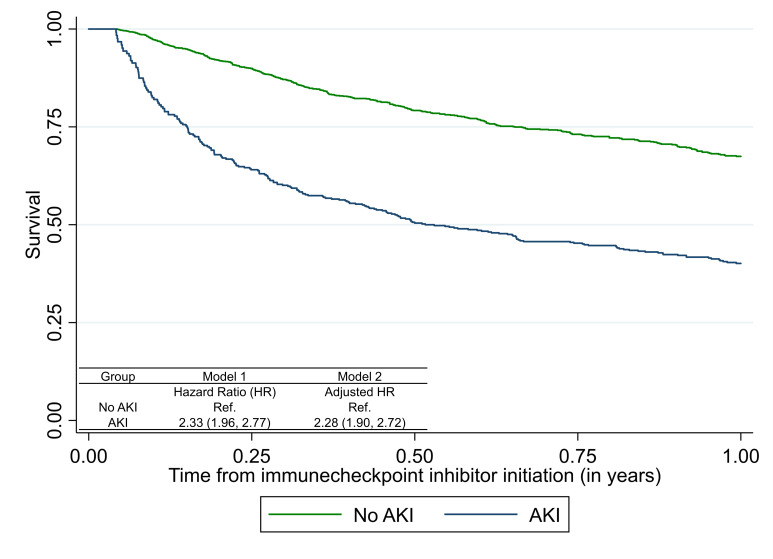
Methods: In this observational cohort study, we included participants initiated on ICI therapy between 2013 and 2019. We tested the independent association of AKI and estimated AIN (eAIN) with mortality up to 1 year after therapy initiation as compared with those without AKI using time-varying Cox proportional hazard models controlling for demographics, comorbidities, cancer type, stage, and therapy, and baseline laboratory values. We defined eAIN as those with a predicted probability of AIN >90th percentile derived from a recently validated diagnostic model.
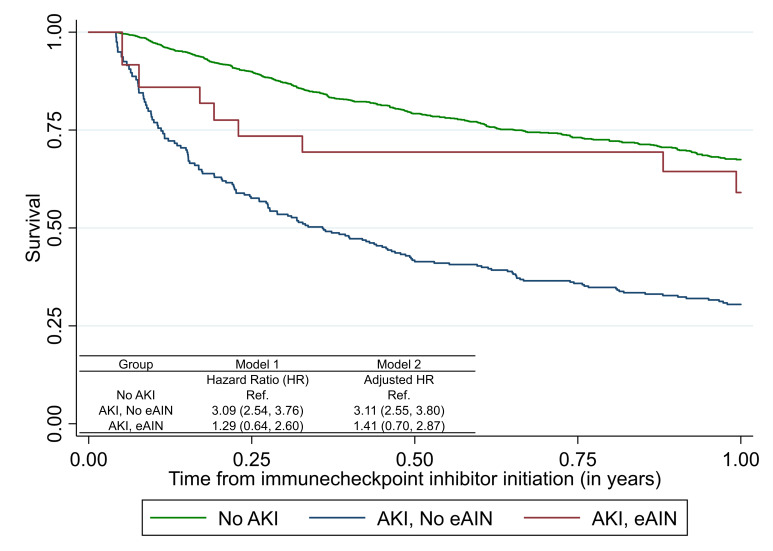
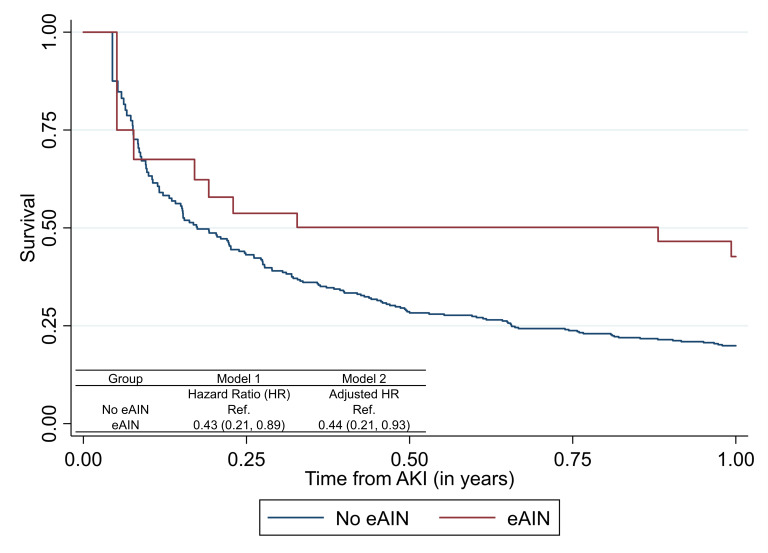
Results: Of 2207 patients initiated on ICIs, 617 (28%) died at 1 year and 549 (25%) developed AKI. AKI was independently associated with higher mortality (adjusted HR, 2.28 (95% CI 1.90 to 2.72)). Those AKI patients with eAIN had more severe AKI as reflected by a higher peak serum creatinine (3.3 (IQR 2.1-6.1) vs 1.4 (1.2-1.9) mg/dL, p<0.001) but exhibited lower mortality than those without eAIN in univariable analysis (HR 0.43 (95% CI 0.21 to 0.89)) and after adjusting for demographics, comorbidities, and cancer type and severity (adjusted HR 0.44 (95% CI 0.21 to 0.93)).
Conclusion: In patients treated with ICI, mortality was higher in those with AKI unrelated to ICI but lower in those where the underlying etiology was AIN. Future studies could evaluate the association of biopsy-proven or biomarker-proven AIN with mortality in those receiving ICI therapy.
Keywords: Biostatistics; Immunotherapy, Active; Translational Medical Research.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: DGM and CRP are coinventors of the pending patent application 'Methods and Systems for Diagnosis of Acute Interstitial Nephritis' that is subject to an option for a license agreement with Renalytix AI.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources