

External validation of the GRACE risk score and the risk-treatment paradox in patients with acute coronary syndrome
- PMID: 35354660
- PMCID: PMC8969003
- DOI: 10.1136/openhrt-2022-001984
External validation of the GRACE risk score and the risk-treatment paradox in patients with acute coronary syndrome
Abstract
Objectives: To validate the Global Registry of Acute Coronary Events (GRACE) risk score and examine the extent and impact of the risk-treatment paradox in contemporary patients with acute coronary syndrome (ACS).
Methods: Data from 5015 patients with ACS enrolled in the FORCE-ACS registry between January 2015 and December 2019 were used for model validation. The performance of the GRACE risk score for predicting in-hospital and 1-year mortality was evaluated based on indices of model discrimination and calibration. Differences in the delivery of guideline-recommended care among patients who survived hospitalisation (n=4911) per GRACE risk stratum were assessed and the association with postdischarge mortality was examined.
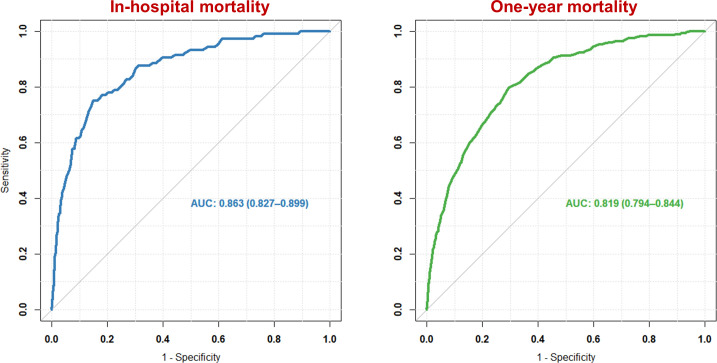
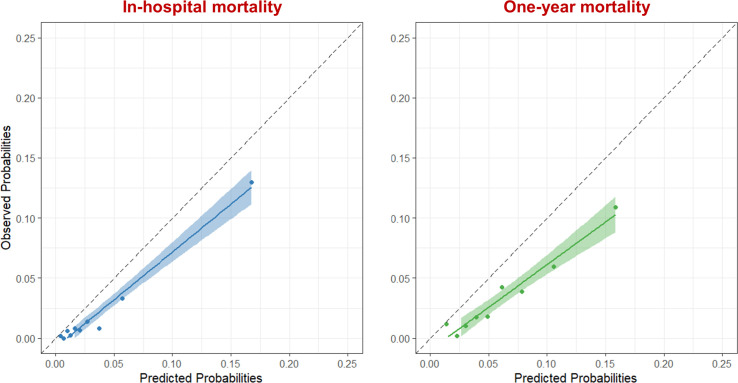
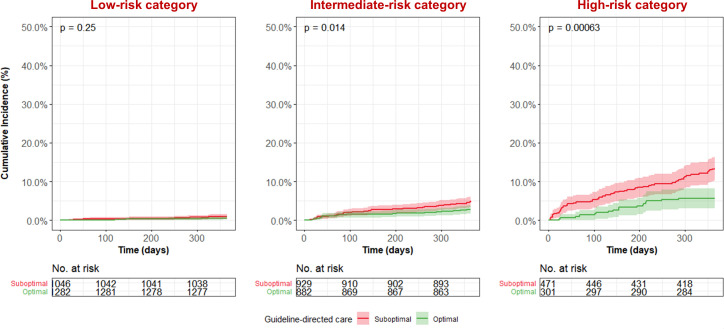
Results: Discriminative power of the GRACE risk score was good for predicting in-hospital (c-statistic: 0.86; 95% CI: 0.83 to 0.90) and 1-year mortality (c-statistic: 0.82; 95% CI: 0.79 to 0.84). However, the GRACE risk score overestimated the absolute in-hospital and 1-year mortality risk (Hosmer-Lemeshow goodness-of-fit test p<0.01). Intermediate-risk and high-risk patients were 12% and 29% less likely to receive optimal guideline-recommended care compared with low-risk patients, respectively. Optimal guideline-recommended care was associated with lower mortality in intermediate- and high-risk patients.
Conclusions: The GRACE risk score identified patients at higher risk for in-hospital and 1-year mortality, but overestimated absolute risk levels in contemporary patients. Optimal guideline-recommended care was associated with lower mortality in intermediate-risk and high-risk patients, but was less likely to be delivered with increasing mortality risk.
Trial registration: ClinicalTrials.gov NCT03823547.
Keywords: acute coronary syndrome; myocardial infarction; pharmacology, clinical.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: Dr Wouter J Kikkert has received a research grant from AstraZeneca. Dr Georgios J Vlachojannis has research grants from MicroPort and Ferrer and personal fees from Terumo and AstraZeneca. Dr Yolande Appelman has received a research grant from the Dutch Heart Foundation. Professor Dr José PS Henriques has received research grants from Abbott Vascular, AstraZeneca, B. Braun, Getinge, Ferrer, Infraredx and ZonMw. Professor Dr Jurriën M ten Berg has received research grants from AstraZeneca and ZonMw and personal fees from AstraZeneca, Accu-Metrics, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, Daiichi Sankyo, Eli Lilly, Ferrer, Idorsia, Pfizer and The Medicines Company. All other authors have no relationships with industry to disclose.
Figures
References
-
- Ibanez B, James S, Agewall S, et al. 2017 ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the task force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of cardiology (ESC). Eur Heart J 2018;39:119–77. 10.1093/eurheartj/ehx393 - DOI - PubMed
-
- Szummer K, Wallentin L, Lindhagen L, et al. Improved outcomes in patients with ST-elevation myocardial infarction during the last 20 years are related to implementation of evidence-based treatments: experiences from the SWEDEHEART registry 1995-2014. Eur Heart J 2017;38:3056–65. 10.1093/eurheartj/ehx515 - DOI - PMC - PubMed
-
- Szummer K, Wallentin L, Lindhagen L, et al. Relations between implementation of new treatments and improved outcomes in patients with non-ST-elevation myocardial infarction during the last 20 years: experiences from SWEDEHEART registry 1995 to 2014. Eur Heart J 2018;39:3766–76. 10.1093/eurheartj/ehy554 - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical