Mild hypoxic-ischemic encephalopathy (HIE): timing and pattern of MRI brain injury
- PMID: 35354930
- PMCID: PMC9771796
- DOI: 10.1038/s41390-022-02026-7
Mild hypoxic-ischemic encephalopathy (HIE): timing and pattern of MRI brain injury
Abstract
Background: Mild hypoxic-ischemic encephalopathy (HIE) is increasingly recognized as a risk factor for neonatal brain injury. We examined the timing and pattern of brain injury in mild HIE.
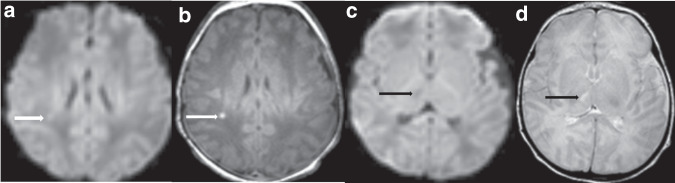
Methods: This retrospective cohort study includes infants with mild HIE treated at 9 hospitals. Neonatal brain MRIs were scored by 2 reviewers using a validated classification system, with discrepancies resolved by consensus. Severity and timing of MRI brain injury (i.e., acute, subacute, chronic) was scored on the subset of MRIs that were performed at or before 8 days of age.
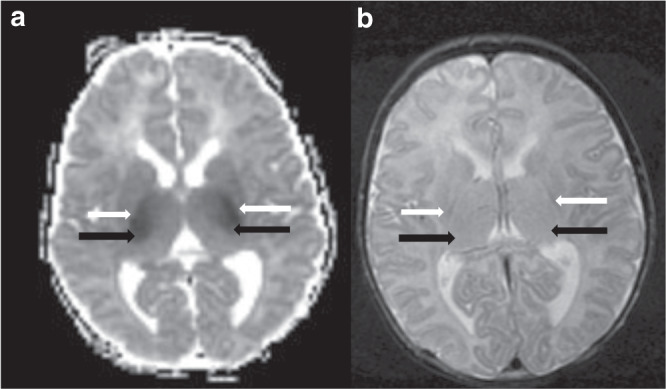
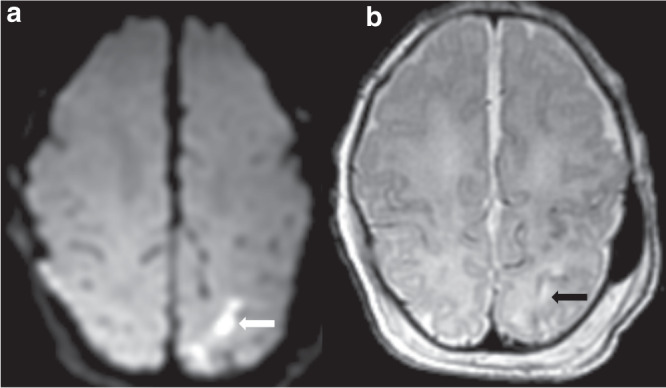
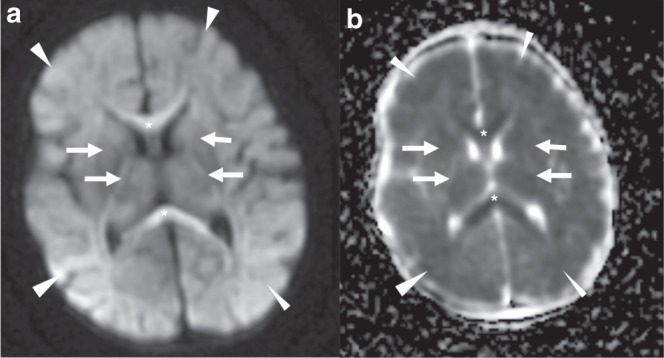
Results: Of 142 infants with mild HIE, 87 (61%) had injury on MRI at median age 5 (IQR 4-6) days. Watershed (23%), deep gray (20%) and punctate white matter (18%) injury were most common. Among the 125 (88%) infants who received a brain MRI at ≤8 days, mild (44%) injury was more common than moderate (11%) or severe (4%) injury. Subacute (37%) lesions were more commonly observed than acute (32%) or chronic lesions (1%).
Conclusion: Subacute brain injury is common in newborn infants with mild HIE. Novel neuroprotective treatments for mild HIE will ideally target both subacute and acute injury mechanisms.
Impact: Almost two-thirds of infants with mild HIE have evidence of brain injury on MRI obtained in the early neonatal period. Subacute brain injury was seen in 37% of infants with mild HIE. Neuroprotective treatments for mild HIE will ideally target both acute and subacute injury mechanisms.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures