

A risk score for predicting death in COVID-19 in-hospital infection: A Brazilian single-center study
- PMID: 35355290
- PMCID: PMC9088307
- DOI: 10.1002/jcu.23195
A risk score for predicting death in COVID-19 in-hospital infection: A Brazilian single-center study
Abstract
Background: There is a paucity of information about Brazilian COVID-19 in-hospital mortality probability of death combining risk factors.
Objective: We aimed to correlate COVID-19 Brazilian in-hospital patients' mortality to demographic aspects, biomarkers, tomographic, echocardiographic findings, and clinical events.
Methods: A prospective study, single tertiary center in Brazil, consecutive patients hospitalized with COVID-19. We analyzed the data from 111 patients from March to August 2020, performed a complete transthoracic echocardiogram, chest thoracic tomographic (CT) studies, collected biomarkers and correlated to in-hospital mortality.
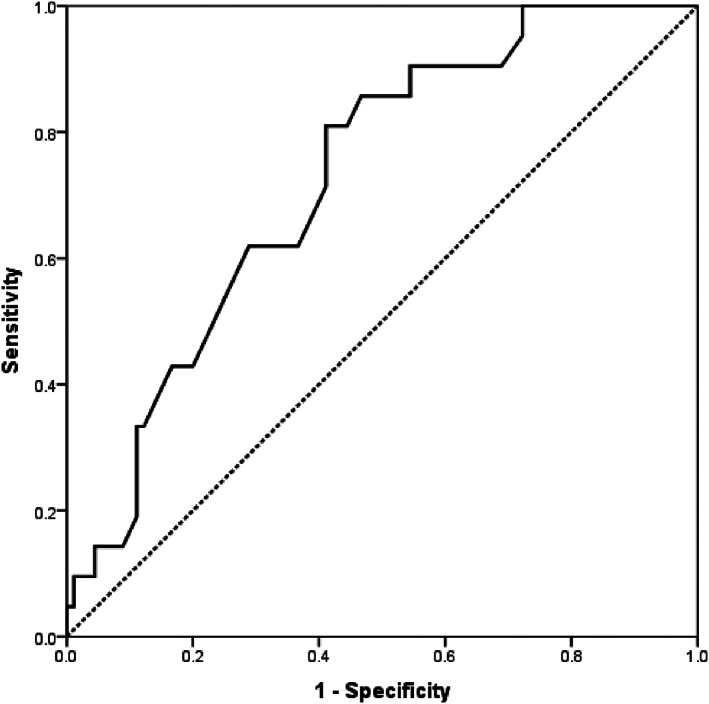
Results: Mean age of the patients: 67 ± 17 years old, 65 (58.5%) men, 29 (26%) presented with systemic arterial hypertension, 18 (16%) with diabetes, 11 (9.9%) with chronic obstructive pulmonary disease. There was need for intubation and mechanical ventilation of 48 (43%) patients, death occurred in 21/111 (18.9%) patients. Multiple logistic regression models correlated variables with mortality: age (OR: 1.07; 95% CI 1.02-1.12; p: 0.012; age >74 YO AUC ROC curve: 0.725), intubation need (OR: 23.35; 95% CI 4.39-124.36; p < 0.001), D dimer (OR: 1.39; 95% CI 1.02-1.89; p: 0.036; value >1928.5 ug/L AUC ROC curve: 0.731), C-reactive protein (OR: 1.18; 95% CI 1.05-1.32; p < 0.005; value >29.35 mg/dl AUC ROC curve: 0.836). A risk score was created to predict intrahospital probability of death, by the equation: 3.6 (age >75 YO) + 66 (intubation need) + 28 (C-reactive protein >29) + 2.2 (D dimer >1900).
Conclusions: A novel and original risk score were developed to predict the probability of death in Covid 19 in-hospital patients concerning combined risk factors.
Keywords: COVID-19; in-hospital patients; mortality.
© 2022 Wiley Periodicals LLC.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
