

Red Flags, Prognostic Impact, and Management of Patients With Cardiac Amyloidosis and Aortic Valve Stenosis: A Systematic Review and Meta-Analysis
- PMID: 35355593
- PMCID: PMC8959832
- DOI: 10.3389/fmed.2022.858281
Red Flags, Prognostic Impact, and Management of Patients With Cardiac Amyloidosis and Aortic Valve Stenosis: A Systematic Review and Meta-Analysis
Abstract
Background: Cardiac amyloidosis (CA) has been recently recognized as a condition frequently associated with aortic stenosis (AS). The aim of this study was to evaluate: the main characteristics of patients with AS with and without CA, the impact of CA on patients with AS mortality, and the effect of different treatment strategies on outcomes of patients with AS with concomitant CA.
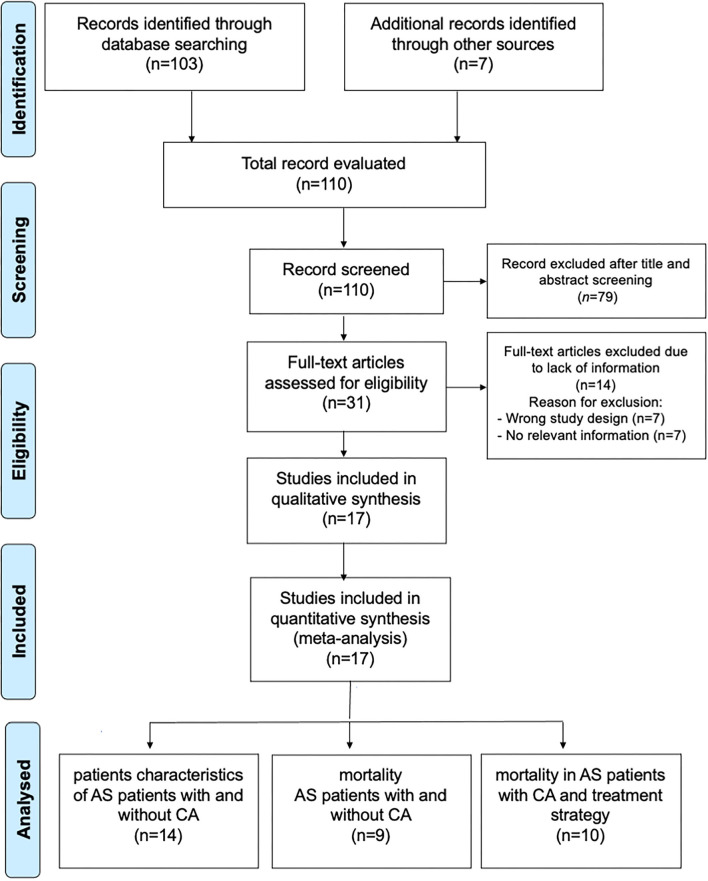
Materials and methods: A detailed search related to CA in patients with AS and outcomes was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Seventeen studies enrolling 1,988 subjects (1,658 AS alone and 330 AS with CA) were included in the qualitative and quantitative analysis of main patients with AS characteristics with and without CA, difference in mortality, and treatment strategy.
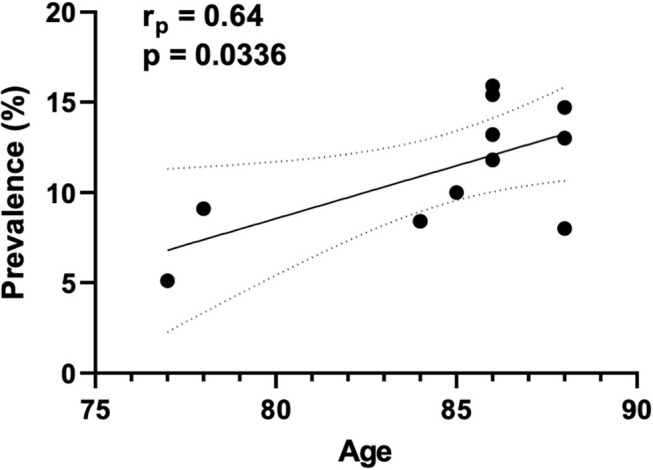
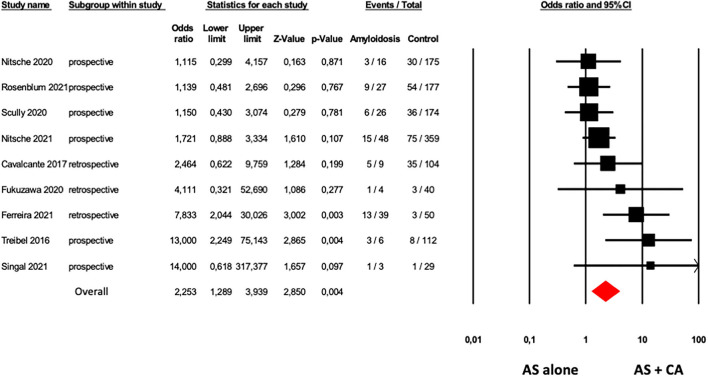
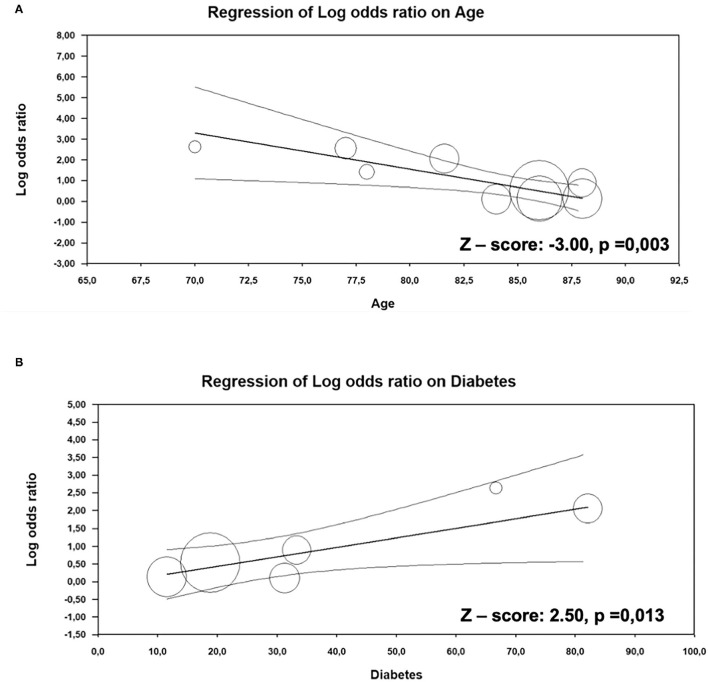
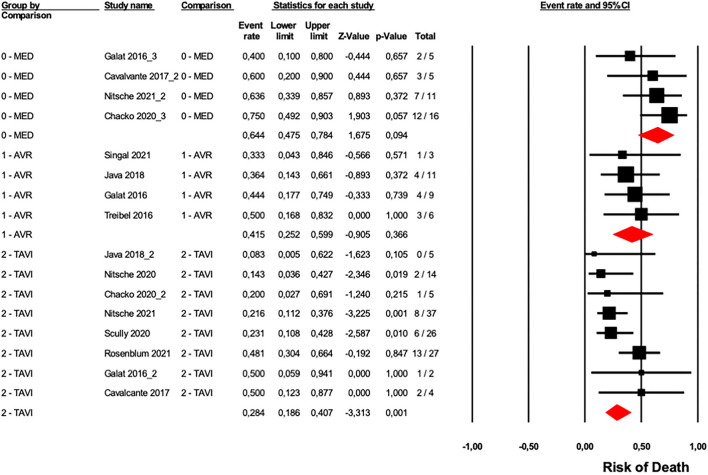
Results: The prevalence of CA resulted in a mean of 15.4% and it was even higher in patients with AS over 80 years old (18.2%). Patients with the dual diagnosis were more often males, had lower body mass index (BMI), were more prone to have low flow, low gradient with reduced left ventricular ejection fraction AS phenotype, had higher E/A and E/e', and greater interventricular septum hypertrophy. Lower Sokolow-Lyon index, higher QRS duration, higher prevalence of right bundle branch block, higher levels of N-terminal pro-brain natriuretic peptide, and high-sensitivity troponin T were significantly associated with CA in patients with AS. Higher overall mortality in the 178 patients with AS + CA in comparison to 1,220 patients with AS alone was observed [odds ratio (OR) 2.25, p = 0.004]. Meta-regression analysis showed that younger age and diabetes were associated with overall mortality in patients with CS with CA (Z-value -3.0, p = 0.003 and Z-value 2.5, p = 0.013, respectively). Finally, patients who underwent surgical aortic valve replacement (SAVR) or transcatheter aortic valve implantation (TAVI) had a similar overall mortality risk, but lower than medication-treated only patients.
Conclusion: Results from our meta-analysis suggest that several specific clinical, electrocardiographic, and echocardiographic features can be considered "red flags" of CA in patients with AS. CA negatively affects the outcome of patients with AS. Patients with concomitant CA and AS benefit from SAVR or TAVI.
Keywords: aortic stenosis (AS); cardiac amyloidosis (CA); outcome; surgical aortic valve replacement; transcatheter aortic valve implantation (TAVI).
Copyright © 2022 Myasoedova, Conte, Valerio, Moschetta, Massaiu, Petraglia, Leosco, Poggio and Parisi.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Prevalence and outcomes of concomitant cardiac amyloidosis and aortic stenosis: A systematic review and meta-analysis.Hellenic J Cardiol. 2022 Mar-Apr;64:67-76. doi: 10.1016/j.hjc.2021.11.001. Epub 2021 Nov 29. Hellenic J Cardiol. 2022. PMID: 34856378
-
A meta-analysis of effects of transcatheter versus surgical aortic valve replacement on left ventricular ejection fraction and mass.Int J Cardiol. 2017 Jul 1;238:31-36. doi: 10.1016/j.ijcard.2017.03.156. Epub 2017 Apr 6. Int J Cardiol. 2017. PMID: 28408105
-
Need for permanent pacemaker as a complication of transcatheter aortic valve implantation and surgical aortic valve replacement in elderly patients with severe aortic stenosis and similar baseline electrocardiographic findings.JACC Cardiovasc Interv. 2012 May;5(5):540-551. doi: 10.1016/j.jcin.2012.03.004. JACC Cardiovasc Interv. 2012. PMID: 22625193
-
Prognostic Impact of Underweight (Body Mass Index <20 kg/m2) in Patients With Severe Aortic Valve Stenosis Undergoing Transcatheter Aortic Valve Implantation or Surgical Aortic Valve Replacement (from the German Aortic Valve Registry [GARY]).Am J Cardiol. 2020 Aug 15;129:79-86. doi: 10.1016/j.amjcard.2020.05.002. Epub 2020 May 13. Am J Cardiol. 2020. PMID: 32540167
-
The predictive value of baseline pulmonary hypertension in early and long term cardiac and all-cause mortality after transcatheter aortic valve implantation for patients with severe aortic valve stenosis: A systematic review and meta-analysis.Cardiovasc Revasc Med. 2018 Oct-Nov;19(7 Pt B):859-867. doi: 10.1016/j.carrev.2018.03.015. Epub 2018 Mar 23. Cardiovasc Revasc Med. 2018. PMID: 29724516
Cited by
-
Valvular heart disease in patients with cardiac amyloidosis.Heart Fail Rev. 2024 Jan;29(1):65-77. doi: 10.1007/s10741-023-10350-1. Epub 2023 Sep 22. Heart Fail Rev. 2024. PMID: 37735319 Free PMC article. Review.
-
Isolated Valve Amyloid Deposition in Aortic Stenosis: Potential Clinical and Pathophysiological Relevance.Int J Mol Sci. 2024 Jan 18;25(2):1171. doi: 10.3390/ijms25021171. Int J Mol Sci. 2024. PMID: 38256243 Free PMC article.
-
A commentary on 'Meta-analysis of post-transcatheter aortic valve replacement outcomes in patients with cardiac amyloidosis and aortic stenosis'.Int J Surg. 2024 Jul 1;110(7):4418-4419. doi: 10.1097/JS9.0000000000001271. Int J Surg. 2024. PMID: 39042089 Free PMC article. No abstract available.
-
The use of deformation imaging in the assessment of patients pre and post transcatheter aortic valve implantation.Echo Res Pract. 2023 Feb 22;10(1):3. doi: 10.1186/s44156-023-00017-w. Echo Res Pract. 2023. PMID: 36810286 Free PMC article.
-
A wolf in sheep's clothing-aortic stenosis and cardiac amyloidosis: "RAISE"ing awareness in clinical practice.Front Cardiovasc Med. 2024 Feb 23;11:1323023. doi: 10.3389/fcvm.2024.1323023. eCollection 2024. Front Cardiovasc Med. 2024. PMID: 38464842 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials