

Treatments for Periductal Mastitis: Systematic Review and Meta-Analysis
- PMID: 35355704
- PMCID: PMC8914206
- DOI: 10.1159/000514419
Treatments for Periductal Mastitis: Systematic Review and Meta-Analysis
Abstract
Introduction: Periductal mastitis (PDM) is a complex benign breast disease with a prolonged course and a high risk of recurrence after treatment. There are many available treatments for PDM, but none is widely accepted. This study aims to evaluate the various treatment failure rates (TFR) of different invasive treatment measures by looking at recurrence and persistence after treatment. In this way, it sets out to inform better clinical decisions in the treatment of PDM.
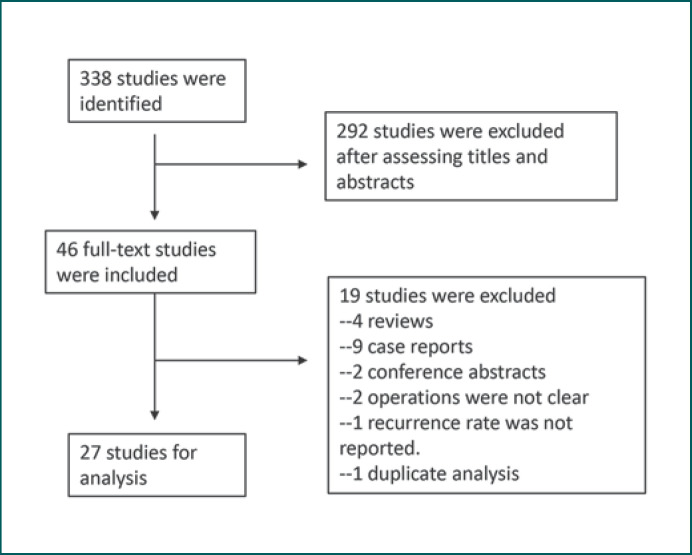
Methods: We searched PubMed, Embase, and Cochrane Library databases for eligible studies about different treatment regimens provided to PDM patients that had been published before October 1, 2019. We included original studies written in English that reported the recurrence and/or persistence rates of each therapy. Outcomes were presented as pooled TFR and 95% CI for the TFR.
Results: We included 27 eligible studies involving 1,066 patients in this study. We summarized 4 groups and 10 subgroups of PDM treatments, according to the published studies. Patients treated minimally invasively (group 1) were subdivided into 3 subgroups and pooled TFR were calculated as follows: incision and drainage (n = 73; TFR = 75.6%; 95% CI 27.3-100%), incision alone (n = 74; TFR = 20.1%; 95% CI 0-59.9%), and breast duct irrigation (n = 123; TFR = 19.4%; 95% CI 0-65.0%). Patients treated with a minor excision (excision of the infected tissue and related duct; group 2) were divided into 4 subgroups and pooled TFR were calculated as follows: wound packing alone (n = 127; TFR = 2.1%; 95% CI 0-5.2%), primary closure alone (n = 66; TFR = 37.1%; 95% CI 9.5-64.8%), primary closure under antibiotic treatment cover (n = 55; TFR = 4.8%; 95% CI 0-11.4%), and additional nipple part removal (n = 232; TFR = 9.6%; 95% CI 5.8-13.4%). Patients treated with a major excision (excision of the infected tissue and the major duct; group 3) included the following 2 subgroups: patients treated with a circumareolar incision (n = 142; TFR = 7.5%; 95% CI 0.4-14.7%) and patients treated with a radial incision of the breast (n = 78; TFR = 0.6%; 95% CI 0-3.6%). Group 4 contained patients receiving different major plastic surgeries. The pooled TFR of this group (n = 86) was 3.4% (95% CI 0-7.5%).
Conclusion: Breast duct irrigation, which is the most minimally invasive of all of the treatment options, seemed to yield good outcomes and may be the first-line treatment for PDM patients. Minor excision methods, except for primary closure alone, might be enough for most PDM patients. Major excision, especially with radial incision, was a highly effective salvage therapy. The major plastic surgery technique was also acceptable as an alternative treatment for patients with large lesions and concerns about breast appearance. Incision and drainage and minor excision with primary closure alone should be avoided for PDM patients. Further research is still needed to better understand the etiology and pathogenesis of PDM and explore more effective treatments for this disease.
Keywords: Failure treatment; Meta-analysis; Periductal mastitis; Recurrence rate; Treatment.
Copyright © 2021 by S. Karger AG, Basel.
Conflict of interest statement
The authors have no conflict of interests to declare.
Similar articles
-
High cure rate and satisfaction in patients with periductal mastitis via the latissimus dorsi myocutaneous flap technique: a retrospective study.Gland Surg. 2024 Jun 30;13(6):794-801. doi: 10.21037/gs-23-484. Epub 2024 Jun 21. Gland Surg. 2024. PMID: 39015716 Free PMC article.
-
Identification of periductal mastitis and granulomatous lobular mastitis: a literature review.Ann Transl Med. 2023 Feb 15;11(3):158. doi: 10.21037/atm-22-6473. Epub 2023 Feb 3. Ann Transl Med. 2023. PMID: 36846004 Free PMC article. Review.
-
Clinical characteristics, classification and surgical treatment of periductal mastitis.J Thorac Dis. 2018 Apr;10(4):2420-2427. doi: 10.21037/jtd.2018.04.22. J Thorac Dis. 2018. PMID: 29850148 Free PMC article.
-
Duct Ectasia and Periductal Mastitis in Indian Women.Indian J Surg. 2015 Dec;77(Suppl 3):957-62. doi: 10.1007/s12262-014-1079-5. Epub 2014 May 8. Indian J Surg. 2015. PMID: 27011490 Free PMC article.
-
Periductal mastitis/duct ectasia.World J Surg. 1989 Nov-Dec;13(6):715-20. doi: 10.1007/BF01658420. World J Surg. 1989. PMID: 2696225 Review.
Cited by
-
High cure rate and satisfaction in patients with periductal mastitis via the latissimus dorsi myocutaneous flap technique: a retrospective study.Gland Surg. 2024 Jun 30;13(6):794-801. doi: 10.21037/gs-23-484. Epub 2024 Jun 21. Gland Surg. 2024. PMID: 39015716 Free PMC article.
-
Mendelian randomization suggests causal correlations between inflammatory cytokines and immune cells with mastitis.Front Immunol. 2024 Sep 27;15:1409545. doi: 10.3389/fimmu.2024.1409545. eCollection 2024. Front Immunol. 2024. PMID: 39399489 Free PMC article.
-
Diagnostic value of radiomics model based on gray-scale and contrast-enhanced ultrasound for inflammatory mass stage periductal mastitis/duct ectasia.Front Oncol. 2022 Sep 20;12:981106. doi: 10.3389/fonc.2022.981106. eCollection 2022. Front Oncol. 2022. PMID: 36203455 Free PMC article.
-
Development of a machine learning-based diagnostic model using hematological parameters to differentiate periductal mastitis from granulomatous lobular mastitis.Sci Prog. 2025 Apr-Jun;108(2):368504251333513. doi: 10.1177/00368504251333513. Epub 2025 Apr 13. Sci Prog. 2025. PMID: 40223288 Free PMC article.
-
Identification of periductal mastitis and granulomatous lobular mastitis: a literature review.Ann Transl Med. 2023 Feb 15;11(3):158. doi: 10.21037/atm-22-6473. Epub 2023 Feb 3. Ann Transl Med. 2023. PMID: 36846004 Free PMC article. Review.
References
-
- Hughes LE. Non-lactational inflammation and duct ectasia. Br Med Bull. 1991 Apr;47((2)):272–283. - PubMed
-
- Zuska JJ, Crile G, Jr, Ayres WW. Fistulas of lactifierous ducts. Am J Surg. 1951 Mar;81((3)):312–317. - PubMed
-
- Dixon JM. Periductal mastitis/duct ectasia. World J Surg. 1989 Nov-Dec;13((6)):715–720. - PubMed
LinkOut - more resources
Full Text Sources
