

Cysteine-Rich Whey Protein Isolate (CR-WPI) Ameliorates Erectile Dysfunction by Diminishing Oxidative Stress via DDAH/ADMA/NOS Pathway
- PMID: 35355865
- PMCID: PMC8960025
- DOI: 10.1155/2022/8151917
Cysteine-Rich Whey Protein Isolate (CR-WPI) Ameliorates Erectile Dysfunction by Diminishing Oxidative Stress via DDAH/ADMA/NOS Pathway
Abstract
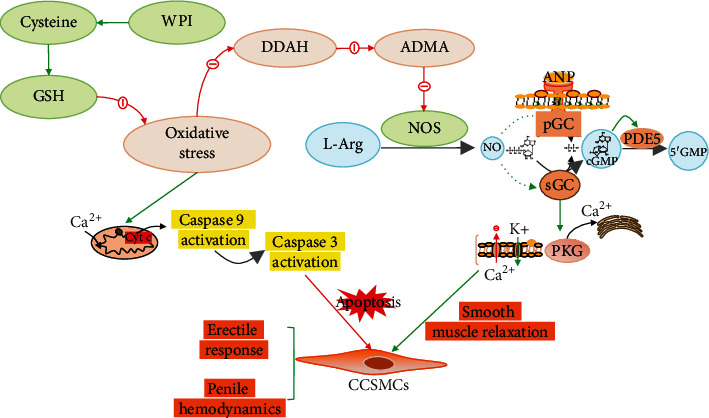
Nitric oxide synthase- (NOS-) dependent endothelial dysfunction induced by oxidative stress (OS) is assumed to play a pivotal role in the pathogenesis and progression of diabetes mellitus-related erectile dysfunction (DMED). Cysteine-rich whey protein isolate (CR-WPI) is a widely used protein supplement and has been confirmed to reduce reactive oxygen species (ROS) by increasing cellular antioxidant glutathione (GSH). However, it is currently unknown whether CR-WPI elicits therapeutic effects in DMED. Here, we provide diabetic rats with CR-WPI to determine its effect on DMED and the underlying mechanisms. The results suggest that CR-WPI supplementation increased GSH biosynthesis and reduced ROS content and simultaneously upregulated the dimethylarginine dimethylaminohydrolase (DDAH)/asymmetrical dimethylarginine (ADMA)/nitric oxide synthase (NOS) metabolic pathway. Evaluation of intracavernous pressure (ICP) also showed an improvement of penile erectile function in CR-WPI-treated rats. The results of the vitro cell culture showed that glutathione pretreatment protected corpus cavernosum smooth muscle cells (CCSMC) from H2O2-induced apoptosis by decreasing Caspase 9 and Caspase 3 expressions. These results augur well for the potential therapeutic application of dietary CR-WPI supplementation for treating diabetic erectile dysfunction.
Copyright © 2022 Kefan Li et al.
Conflict of interest statement
Jimmy Gutman consults with a whey protein distributor.
Figures





References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
