

From the Ground Up: Esophageal Atresia Types, Disease Severity Stratification and Survival Rates at a Single Institution
- PMID: 35356503
- PMCID: PMC8959439
- DOI: 10.3389/fsurg.2022.799052
From the Ground Up: Esophageal Atresia Types, Disease Severity Stratification and Survival Rates at a Single Institution
Abstract
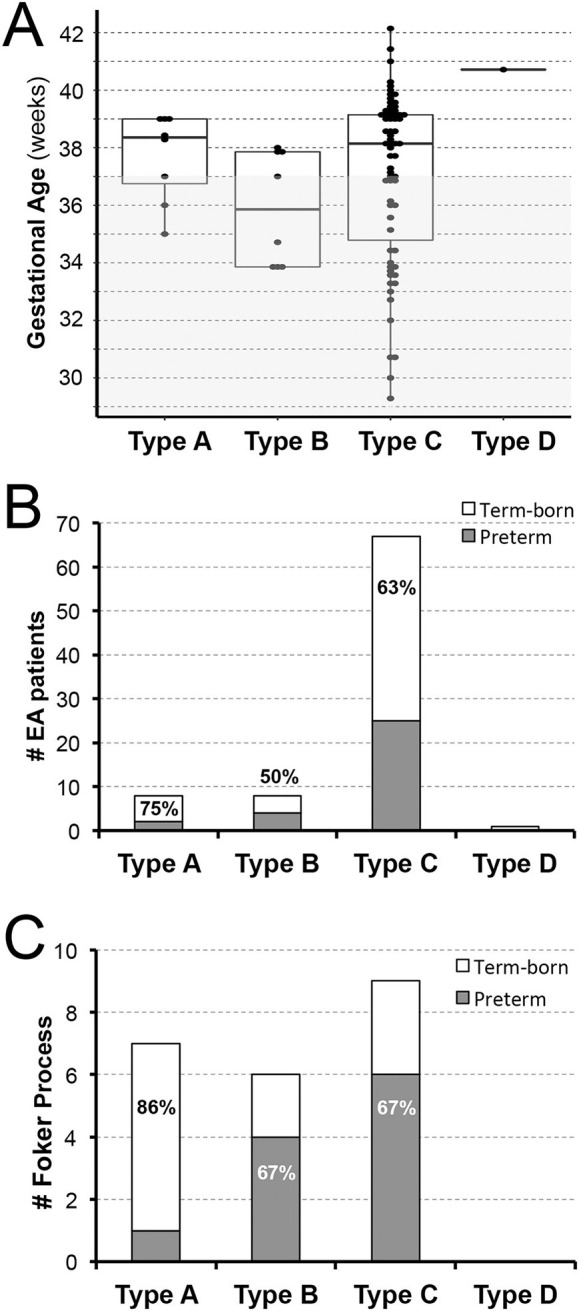
Esophageal atresia (EA), although a rare congenital anomaly, represents one of the most common gastrointestinal birth defects. There is a gap in our knowledge regarding the impact of perioperative critical care in infants born with EA. This study addresses EA types, disease severity stratification, and mortality in a retrospective cohort at a single institution. Institutional Review Board approved our retrospective cross-sectional study of term-born (n = 53) and premature infants (28-37 weeks of gestation; n = 31) that underwent primary surgical repair of EA at a single institution from 2009-2020. Demographic and clinical data were obtained from the electronic medical record, Powerchart (Cerner, London, UK). Patients were categorized by (i) sex, (ii) gestational age at birth, (iii) types of EA (in relation to respiratory tract anomalies), (iv) co-occurring congenital anomalies, (v) severity of disease (viz. American Society of Anesthesiologists (ASA) and Pediatric Risk Assessment (PRAm) scores), (vi) type of surgical repair for EA (primary anastomosis vs. Foker process), and (vii) survival rate classification using Spitz and Waterston scores. Data were presented as numerical sums and percentages. The frequency of anatomical types of EA in our cohort parallels that of the literature: 9.5% (8/84) type A, 9.5% (8/84) type B, 80% (67/84) type C, and 1% (1/84) type D. Long-gap EA accounts for 88% (7/8) type A, 75% (6/8) type B, and 13% (9/67) type C in the cohort studied. Our novel results show a nearly equal distribution of sex per each EA type, and gestational age (term-born vs. premature) by anatomical EA type. PRAm scoring showed a wider range of disease severity (3-9) than ASA scores (III and IV). The survival rate in our EA cohort dramatically increased in comparison to the literature in previous decades. This retrospective analysis at a single institution shows incidence of EA per sex and gestational status for anatomical types (EA type A-D) and by surgical approach (primary anastomosis vs. Foker process for short-gap vs. long-gap EA, respectively). Despite its wider range, PRAm score was not more useful in predicting disease severity in comparison to ASA score. Increased survival rates over the last decade suggest a potential need to assess unique operative and perioperative risks in this unique population of patients. Presented findings also represent a foundation for future clinical studies of outcomes in infants born with EA.
Keywords: ASA; EA; LGEA; PRAm; mortality; premature; term; term-born infant.
Copyright © 2022 Evanovich, Wang, Zendejas, Jennings and Bajic.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures




References
-
- Moore KL, Persaud TVN, Torchia MG. Alimentary System. In Moore KL, Persaud TVN, Torchia MG, editors. The Developing Human: Clinically Oriented Embryology. London: Elsevier India; (2012), p. 193–221. Available online at: https://www.elsevier.com/books/the-developing-human-clinically-oriented-...
-
- Gross RE. The Surgery of Infancy and Childhood: its principles and techniques. Philadelphia, London: WB Saunders; (1953).
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous