

The Challenges of Diagnosing Nondilated Obstructive Uropathy: A Case Report
- PMID: 35356536
- PMCID: PMC8958704
- DOI: 10.1177/20543581221086683
The Challenges of Diagnosing Nondilated Obstructive Uropathy: A Case Report
Abstract
Rationale: Nondilated obstructive uropathy (NDOU) is a rare cause of acute renal failure reported in less than 5% of cases of obstructive uropathy. It is typically associated with intrapelvic malignancies and diseases causing retroperitoneal lymphadenopathy and retroperitoneal fibrosis. As these conditions may prevent radiographic dilation of the collecting system, the diagnosis of NDOU may be missed by usual diagnostic testing.
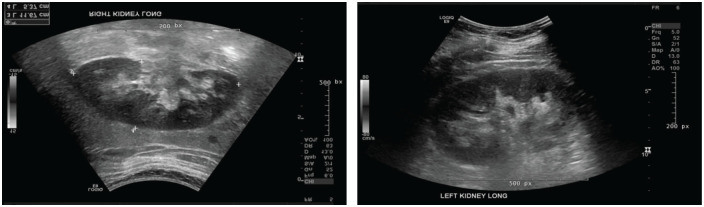
Presenting concerns of the patient: We present a case of acute anuric renal failure in a middle-aged woman with metastatic breast cancer associated with abdominal and retroperitoneal lymphadenopathy. Acute kidney injury was initially deemed secondary to drug-induced acute tubular necrosis (ATN) from bisphosphonate; however, there remained a high clinical suspicion of NDOU due to the presence of enlarged retroperitoneal lymph nodes on CT abdomen and pelvis with concerns for encasement of bilateral renal pelvic regions and ureters.
Diagnoses: The patient underwent a retrograde pyelogram which demonstrated questionable narrowing bilaterally at the level of the renal pelvices. This led to an even stronger clinical suspicion of NDOU and urology service was consulted for evaluation.
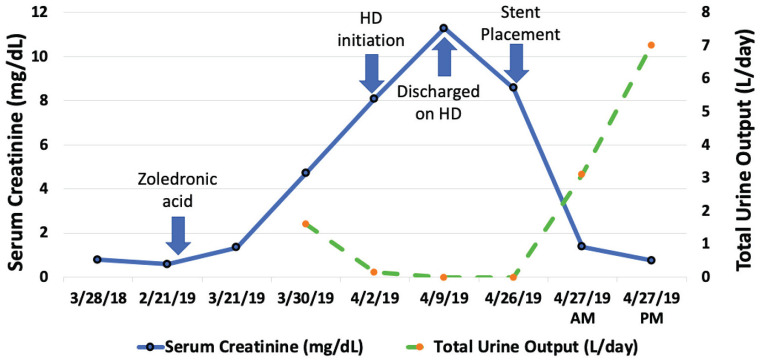
Intervention: Bilateral ureteral stents were placed by urology which led to robust urine output and rapid reversal of renal failure over the next 24 to 48 hours.
Outcomes: Despite 2 weeks of anuria and hemodialysis, this patient's creatinine came back to her baseline. She was able to discontinue hemodialysis and her creatinine stabilized at 88.4 μmol/L (1 mg/dL).
Teaching points: Nondilated obstructive uropathy is rare but important diagnosis that requires a high clinical suspicion in the appropriate clinical scenario. The lack of dilatation is believed to be related to encasement of the collecting system by tumor, fibrosis, or as in our case metastatic retroperitoneal lymphadenopathy. As this diagnosis cannot be overlooked, aggressive direct visualization or even intervention with internal or external stenting may be required to both diagnose and treat this condition.
Justification: L’uropathie obstructive sans dilatation (UOSD) est une cause rare d’insuffisance rénale aiguë (IRA) rapportée dans moins de 5 % des cas d’uropathie obstructive. Elle est généralement associée à des tumeurs malignes intrapelviennes et de maladies entraînant une lymphadénopathie rétropéritonéale et une fibrose rétropéritonéale. Ces conditions pouvant empêcher la dilatation radiographique du système collecteur, il arrive que le diagnostic de l’UOSD soit manqué lors des tests de diagnostic habituels.
Présentation du cas: Nous présentons un cas d’IRA anurique chez une femme d’âge moyen atteinte d’un cancer du sein métastatique associé à une lymphadénopathie abdominale et rétropéritonéale (LAR). L’IRA avait initialement été considérée comme secondaire à une nécrose tubulaire aiguë induite par le bisphosphonate. La présence de ganglions lymphatiques rétropéritonéaux hypertrophiés sur la tomographie de l’abdomen et du bassin a toutefois soulevé un doute clinique d’UOSD; une obstruction des régions bilatérales du bassinet rénal et des uretères a été soupçonné.
Diagnostic: La patiente a subi un pyélogramme rétrograde qui a montré un rétrécissement bilatéral suspect au niveau des bassinets rénaux, ce qui a soulevé un doute clinique encore plus important quant à la présence d’une UOSD. Le service d’urologie a été consulté pour évaluation.
Intervention: Des endoprothèses urétérales ont été insérées bilatéralement par urologie. L’intervention a entraîné une forte production d’urine et la disparition de l’insuffisance rénale dans les 24 à 48 heures suivantes.
Résultats: Malgré deux semaines d’anurie et d’hémodialyse, le taux de créatinine de la patiente est retourné à sa valeur initiale. La patiente a pu interrompre l’hémodialyse et son taux de créatinine s’est stabilisé à 88,4 micromoles/L (1 mg/dl).
Enseignements tirés: Le diagnostic de l’UOSD est rare, mais important, car il requiert un doute clinique élevé dans le scénario clinique approprié. On pense que l’absence de dilatation pourrait être liée à l’obstruction du système collecteur rénal par une tumeur ou en raison d’une fibrose ou, comme ici, d’une lymphadénopathie rétropéritonéale métastatique. Puisque le diagnostic de l’UOSD ne doit pas être négligé, une visualisation directe plus poussée et l’insertion d’une endoprothèse interne ou externe pourraient s’avérer nécessaires pour diagnostiquer et traiter cette affection.
Keywords: acute kidney injury; acute tubular necrosis; obstructive uropathy; retroperitoneal lymphadenopathy.
© The Author(s) 2022.
Conflict of interest statement
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- National Clinical Guideline Centre (UK). Acute Kidney Injury: Prevention, Detection and Management Up to the Point of Renal Replacement Therapy. London, England: Royal College of Physicians (UK); 2013. - PubMed
-
- Onuigbo MA, Lawrence K, Onuigbo NT. Non-dilated obstructive uropathy—an unrecognized cause of acute renal failure in hospitalized US patients: three case reports seen over 6 months in a northwestern Wisconsin nephrology practice. Ren Fail. 2010;32(10):1226-1229. - PubMed
-
- Kocurek JN, Orihuela E, Saltzstein DR. Nondilated obstructive uropathy and renal failure as a result of carcinoma of the intrapelvic area. Surg Gynecol Obstet. 1991;173(6):470-472. - PubMed
-
- Spital A, Valvo JR, Segal AJ. Nondilated obstructive uropathy. Urology. 1988;31(6):478-482. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
