

A systematic review on estimating population attributable fraction for risk factors for small-for-gestational-age births in 81 low- and middle-income countries
- PMID: 35356650
- PMCID: PMC8942297
- DOI: 10.7189/jogh.12.04024
A systematic review on estimating population attributable fraction for risk factors for small-for-gestational-age births in 81 low- and middle-income countries
Abstract
Background: Small for gestational age (SGA) is a public health concern since it is associated with mortality in neonatal and post-neonatal period. Despite the large magnitude of the problem, little is known about the population-attributable risk (PAR) of various risk factors for SGA. This study estimated the relative contribution of risk factors for SGA, as a basis for identifying priority areas for developing and/or implementing interventions to reduce the incidence of SGA births and related mortality and morbidity.
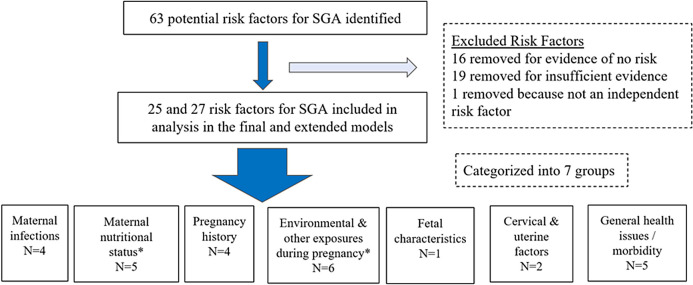
Methods: We conducted a literature review on 63 potential risk factors for SGA to quantify the risk relationship and estimate the prevalence of risk factors (RFs). We calculated the population-attributable fraction for each of the identified RF for 81 Countdown countries and calculated regional estimates. Twenty-five RFs were included in the final model while extended model included all the 25 RFs from the final model and two additional RFs.
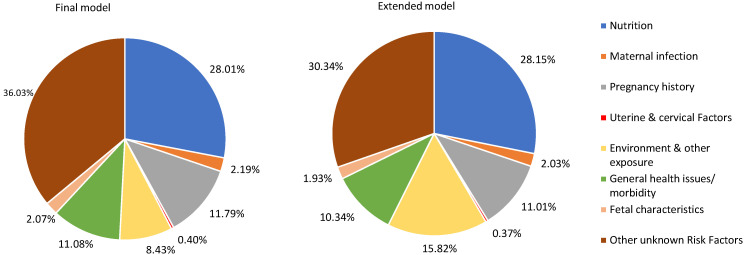
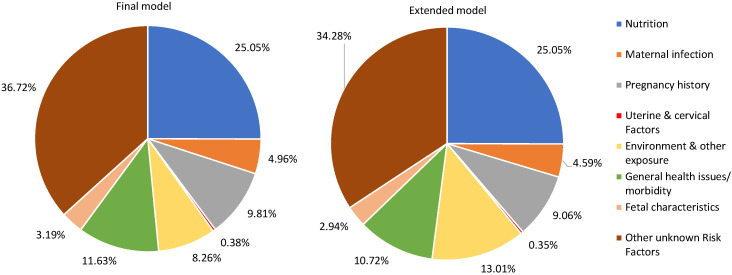
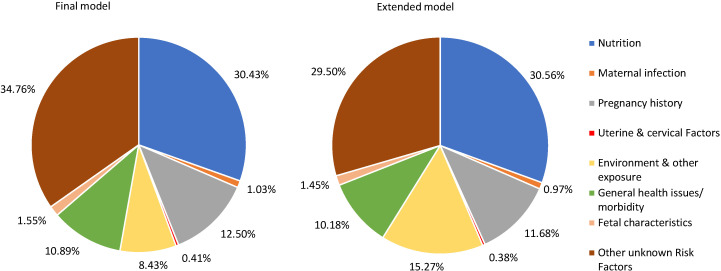
Results: In the final and extended models, the RFs included in each model have a total PAF equal to 63.97% and 69.66%, respectively of SGA across the 81 LMICs. In the extended model, maternal nutritional status has the greatest PAF (28.15%), followed by environmental and other exposures during pregnancy (15.82%), pregnancy history (11.01%), and general health issues or morbidity (10.34%). The RFs included in the final and extended model for Sub-Saharan African (SSA) region have a total PAF of 63.28% and 65.72% of SGA, respectively. In SSA, the top three RF categories in the extended model are nutrition (25.05%), environment and other exposure (13.01%), and general health issues or morbidity (10.72%), while in South-Asia's it was nutrition (30.56%), environment and other exposure (15.27%) and pregnancy history (11.68%).
Conclusions: The various types of RFs that play a role in SGA births highlight the importance of a multifaceted approach to tackle SGA. Depending on the types of RFs, intervention should be strategically targeted at either individual or household and/or community or policy level. There is also a need to research the mechanisms by which some of the RFs might hinder fetal growth.
Copyright © 2022 by the Journal of Global Health. All rights reserved.
Conflict of interest statement
Conflict of interest: The authors completed the ICMJE Unified Competing Interest Form (available upon request from the corresponding author), and declare no conflicts of interest.
Figures
Similar articles
-
New Option in the Lives Saved Tool (LiST) Allows for the Conversion of Prevalence of Small-for-Gestational-Age and Preterm Births to Prevalence of Low Birth Weight.J Nutr. 2017 Nov;147(11):2141S-2146S. doi: 10.3945/jn.117.247767. Epub 2017 Sep 13. J Nutr. 2017. PMID: 28904115 Review.
-
Population attributable fractions for risk factors for spontaneous preterm births in 81 low- and middle-income countries: A systematic analysis.J Glob Health. 2022 Mar 26;12:04013. doi: 10.7189/jogh.12.04013. eCollection 2022. J Glob Health. 2022. PMID: 35356651 Free PMC article. Review.
-
Determinants of low birthweight, small-for-gestational-age and preterm birth in Lombok, Indonesia: analyses of the birthweight cohort of the SUMMIT trial.Trop Med Int Health. 2012 Aug;17(8):938-50. doi: 10.1111/j.1365-3156.2012.03039.x. Trop Med Int Health. 2012. PMID: 22943372 Clinical Trial.
-
Maternal region of origin and Small for gestational age: a cross-sectional analysis of Victorian perinatal data.BMC Pregnancy Childbirth. 2021 May 29;21(1):409. doi: 10.1186/s12884-021-03864-9. BMC Pregnancy Childbirth. 2021. PMID: 34051749 Free PMC article.
-
Demographic, socio-economic, obstetric, and behavioral factors associated with small-and large-for-gestational-age from a prospective, population-based pregnancy cohort in rural Nepal: a secondary data analysis.BMC Pregnancy Childbirth. 2022 Aug 19;22(1):652. doi: 10.1186/s12884-022-04974-8. BMC Pregnancy Childbirth. 2022. PMID: 35986258 Free PMC article. Clinical Trial.
Cited by
-
The impact of enhancing nutrition and antenatal infection treatment on birth outcomes in Amhara, Ethiopia: a pragmatic factorial, cluster-randomised clinical effectiveness study.BMJ Glob Health. 2025 Jun 18;10(6):e016264. doi: 10.1136/bmjgh-2024-016264. BMJ Glob Health. 2025. PMID: 40533249 Free PMC article. Clinical Trial.
-
Integrated multisectoral interventions to mitigate the risk of low birth weight in low- and middle-income country settings: Implementation considerations for programs from a WHO expert consultation.J Glob Health. 2024 Sep 13;14:03033. doi: 10.7189/jogh.14.03033. J Glob Health. 2024. PMID: 39268661 Free PMC article. No abstract available.
-
Comprehensive assessment of the genetic characteristics of small for gestational age newborns in NICU: from diagnosis of genetic disorders to prediction of prognosis.Genome Med. 2023 Dec 13;15(1):112. doi: 10.1186/s13073-023-01268-2. Genome Med. 2023. PMID: 38093364 Free PMC article.
-
The economic burden of perinatal mortality due to inaction on preconception health in low and middle-income countries: A population attributable fraction and economic impact analysis.PLoS One. 2025 Jul 3;20(7):e0325086. doi: 10.1371/journal.pone.0325086. eCollection 2025. PLoS One. 2025. PMID: 40608770 Free PMC article.
-
Socio-economic differences among low-birthweight infants in Hungary. Results of the Cohort '18 -Growing Up in Hungary birth cohort study.PLoS One. 2023 Sep 1;18(9):e0291117. doi: 10.1371/journal.pone.0291117. eCollection 2023. PLoS One. 2023. PMID: 37656714 Free PMC article.
References
-
- Marconi AM, Battaglia F. Intrauterine Growth Restriction: Obstetric Aspects. Neonatology. Springer, Cham. 2012. p. 77–81.
-
- Lee AC, Kozuki N, Cousens S, Stevens GA, Blencowe H, Silveira MF, et al. Estimates of burden and consequences of infants born small for gestational age in low and middle income countries with INTERGROWTH-21st standard: analysis of CHERG datasets. BMJ. 2017;358:j3677. 10.1136/bmj.j3677 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
