

Bipolar androgen therapy (BAT): A patient's guide
- PMID: 35357024
- PMCID: PMC9313844
- DOI: 10.1002/pros.24328
Bipolar androgen therapy (BAT): A patient's guide
Abstract
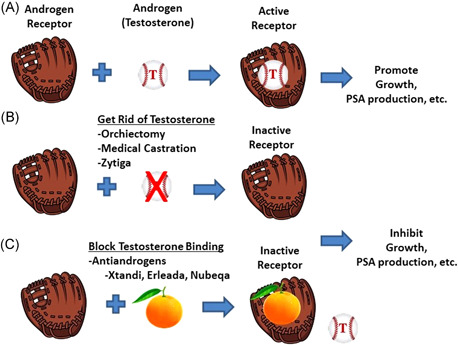
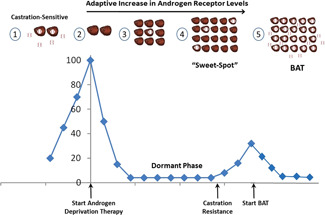
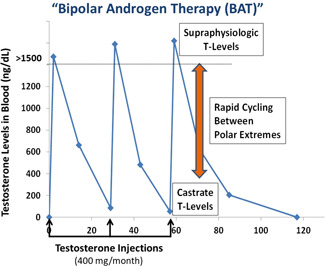
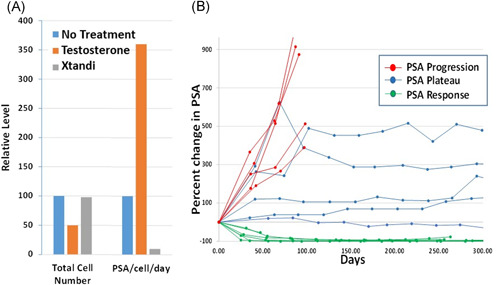
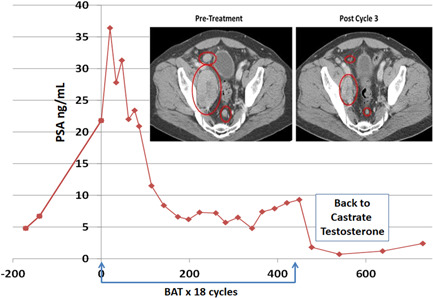
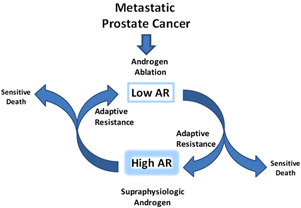
Bipolar androgen therapy (BAT) is a new treatment concept for men whose prostate cancer has become resistant to standard hormone-blocking therapy. Over the past decade, we have performed a series of clinical studies testing BAT in asymptomatic men with castration-resistant prostate cancer. The key findings from these clinical studies are that BAT (a) can be safely administered to asymptomatic patients with metastatic castrate-resistant prostate cancer; (b) does not produce symptomatic disease progression; (c) produces sustained prostate-specific antigen and objective responses in 30%-40% of patients; and (d) can resensitize and prolong response to subsequent antiandrogen therapy. The concept of BAT has generated significant interest from men with prostate cancer, their families, and their physicians. Here we provide a "Patient's Guide" that answers questions about BAT in a form that is accessible to patients, their families, and physicians. Our goal is to provide information to help patients make the most informed decisions they can regarding their prostate cancer treatment.
Keywords: androgen deprivation; antiandrogen; bipolar androgen therapy; castration resistant.
© 2022 The Authors. The Prostate published by Wiley Periodicals LLC.
Figures
Similar articles
-
Bipolar Androgen Therapy for Men With Androgen Ablation Naïve Prostate Cancer: Results From the Phase II BATMAN Study.Prostate. 2016 Sep;76(13):1218-26. doi: 10.1002/pros.23209. Epub 2016 Jun 24. Prostate. 2016. PMID: 27338150 Clinical Trial.
-
Bipolar androgen therapy for treatment of metastatic castration-resistant prostate cancer: A case series.Prostate. 2025 Jan;85(1):40-47. doi: 10.1002/pros.24798. Epub 2024 Sep 22. Prostate. 2025. PMID: 39308006
-
The testosterone paradox of advanced prostate cancer: mechanistic insights and clinical implications.Nat Rev Urol. 2023 May;20(5):265-278. doi: 10.1038/s41585-022-00686-y. Epub 2022 Dec 21. Nat Rev Urol. 2023. PMID: 36543976 Free PMC article. Review.
-
Bipolar androgen therapy sensitizes castration-resistant prostate cancer to subsequent androgen receptor ablative therapy.Eur J Cancer. 2021 Feb;144:302-309. doi: 10.1016/j.ejca.2020.11.043. Epub 2020 Dec 29. Eur J Cancer. 2021. PMID: 33383350 Free PMC article. Clinical Trial.
-
[Bipolar androgen therapy: A novel therapeutic strategy for castration-resistant prostate cancer].Zhonghua Nan Ke Xue. 2017 Dec;23(12):1138-1140. Zhonghua Nan Ke Xue. 2017. PMID: 29738189 Review. Chinese.
Cited by
-
Strategies to Re-Sensitize Castration-Resistant Prostate Cancer to Antiandrogen Therapy.Biomedicines. 2023 Apr 6;11(4):1105. doi: 10.3390/biomedicines11041105. Biomedicines. 2023. PMID: 37189723 Free PMC article. Review.
-
Two Decades of Disease Evolution and Biomarker-Guided Clinical Decision Making in Metastatic Prostate Cancer.Int J Mol Sci. 2025 Aug 6;26(15):7593. doi: 10.3390/ijms26157593. Int J Mol Sci. 2025. PMID: 40806723 Free PMC article.
-
H2AJ Is a Direct Androgen Receptor Target Gene That Regulates Androgen-Induced Cellular Senescence and Inhibits Mesenchymal Markers in Prostate Cancer Cells.Cancers (Basel). 2025 Feb 25;17(5):791. doi: 10.3390/cancers17050791. Cancers (Basel). 2025. PMID: 40075640 Free PMC article.
-
Altered expression of vesicular trafficking machinery in prostate cancer affects lysosomal dynamics and provides insight into the underlying biology and disease progression.Br J Cancer. 2024 Nov;131(8):1263-1278. doi: 10.1038/s41416-024-02829-x. Epub 2024 Aug 31. Br J Cancer. 2024. PMID: 39217195 Free PMC article.
-
Targeting Androgen, Thyroid Hormone, and Vitamin A and D Receptors to Treat Prostate Cancer.Int J Mol Sci. 2024 Aug 26;25(17):9245. doi: 10.3390/ijms25179245. Int J Mol Sci. 2024. PMID: 39273194 Free PMC article. Review.
References
-
- Huggins C. The effects of castration on advanced carcinoma of the prostate gland. Arch Surg. 1941;43:209.
-
- Chuu CP, Hiipakka RA, Fukuchi J, Kokontis JM, Liao S. Androgen causes growth suppression and reversion of androgen‐independent prostate cancer xenografts to an androgen‐stimulated phenotype in athymic mice. Cancer Res. 2005;65:2082‐2084. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
