

Spectacle Lenses With Aspherical Lenslets for Myopia Control vs Single-Vision Spectacle Lenses: A Randomized Clinical Trial
- PMID: 35357402
- PMCID: PMC8972151
- DOI: 10.1001/jamaophthalmol.2022.0401
Spectacle Lenses With Aspherical Lenslets for Myopia Control vs Single-Vision Spectacle Lenses: A Randomized Clinical Trial
Abstract
Importance: Reducing myopia progression can reduce the risk of associated ocular pathologies.
Objective: To evaluate whether spectacle lenses with higher lenslet asphericity have a higher myopia control efficacy throughout 2 years.
Design, setting, and participants: This double-masked randomized clinical trial was conducted between July 2018 and October 2020 at the Eye Hospital of Wenzhou Medical University in Wenzhou, China. Children aged 8 to 13 years with a cycloplegic spherical equivalent refraction (SER) of -0.75 D to -4.75 D and astigmatism with less than -1.50 D were recruited. A data and safety monitoring committee reviewed findings from a planned interim analysis in 2019.
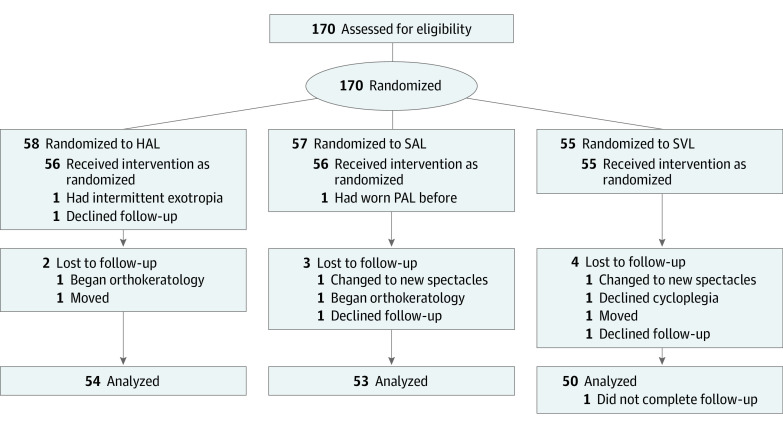
Interventions: Participants were randomly assigned in a 1:1:1 ratio to receive spectacle lenses with highly aspherical lenslets (HAL), spectacle lenses with slightly aspherical lenslets (SAL), or single-vision spectacle lenses (SVL).
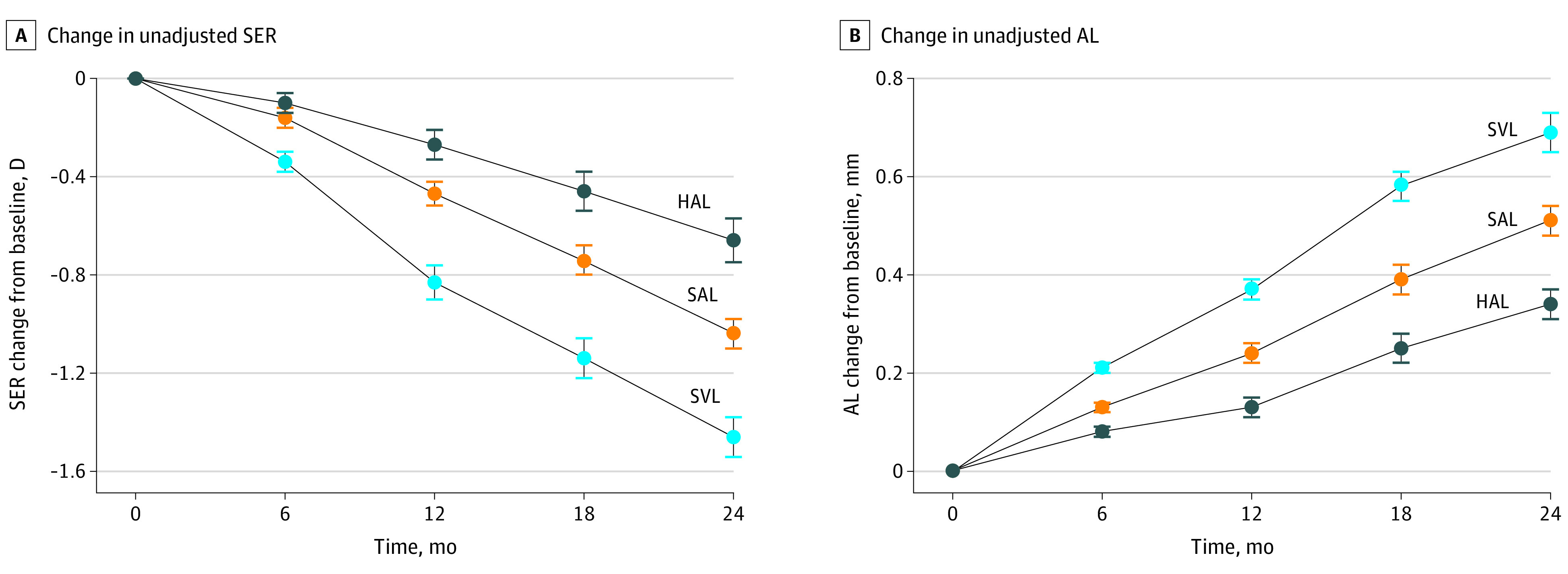
Main outcome and measures: Two-year changes in SER and axial length and their differences between groups.
Results: Of 157 participants who completed each visit (mean [SD] age, 10.4 [1.2] years), 54 were analyzed in the HAL group, 53 in the SAL group, and 50 in the SVL group. Mean (SE) 2-year myopia progression in the SVL group was 1.46 (0.09) D. Compared with SVL, the mean (SE) change in SER was less for HAL (by 0.80 [0.11] D) and SAL (by 0.42 [0.11] D; P ≤ .001). The mean (SE) increase in axial length was 0.69 (0.04) mm for SVL. Compared with SVL, increase in axial length was slowed by a mean (SE) of 0.35 (0.05) mm for HAL and 0.18 (0.05) mm for SAL (P ≤ .001). Compared with SVL, for children who wore HAL at least 12 hours every day, the mean (SE) change in SER was slowed by 0.99 (0.12) D, and increase in axial length slowed by 0.41 (0.05) mm.
Conclusions and relevance: In this study, HAL and SAL reduced the rate of myopia progression and axial elongation throughout 2 years, with higher efficacy for HAL. Longer wearing hours resulted in better myopia control efficacy for HAL.
Trial registration: Chinese Clinical Trial Registry Identifier: ChiCTR1800017683.
Conflict of interest statement
Figures
Comment in
-
Clinical Relevance of Myopia Control With Specialized Spectacles.JAMA Ophthalmol. 2022 May 1;140(5):478-479. doi: 10.1001/jamaophthalmol.2022.0533. JAMA Ophthalmol. 2022. PMID: 35357397 No abstract available.
