

Postoperative mortality risk assessment in colorectal cancer: development and validation of a clinical prediction model using data from the Dutch ColoRectal Audit
- PMID: 35357416
- PMCID: PMC8969795
- DOI: 10.1093/bjsopen/zrac014
Postoperative mortality risk assessment in colorectal cancer: development and validation of a clinical prediction model using data from the Dutch ColoRectal Audit
Abstract
Background: As the outcome of modern colorectal cancer (CRC) surgery has significantly improved over the years, however, renewed and adequate risk stratification for mortality is important to identify high-risk patients. This population-based study was conducted to analyse postoperative outcomes in patients with CRC and to create a risk model for 30-day mortality.
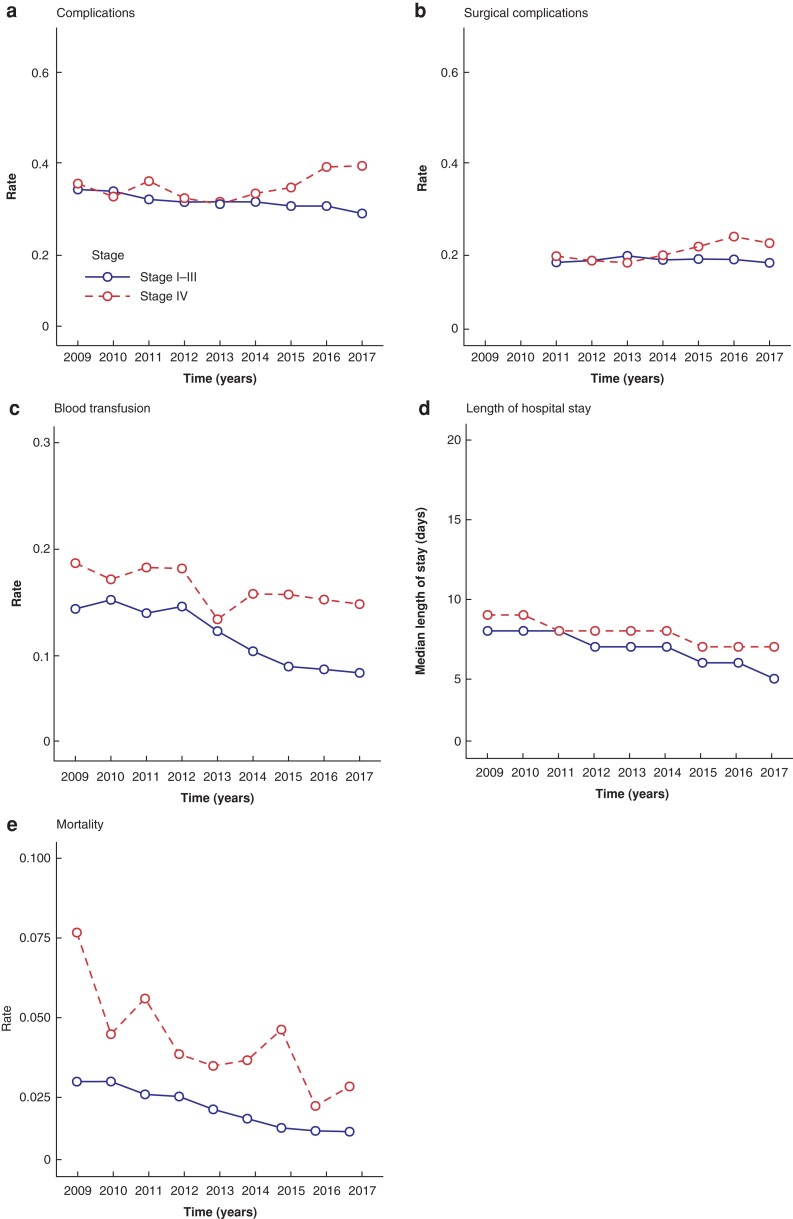
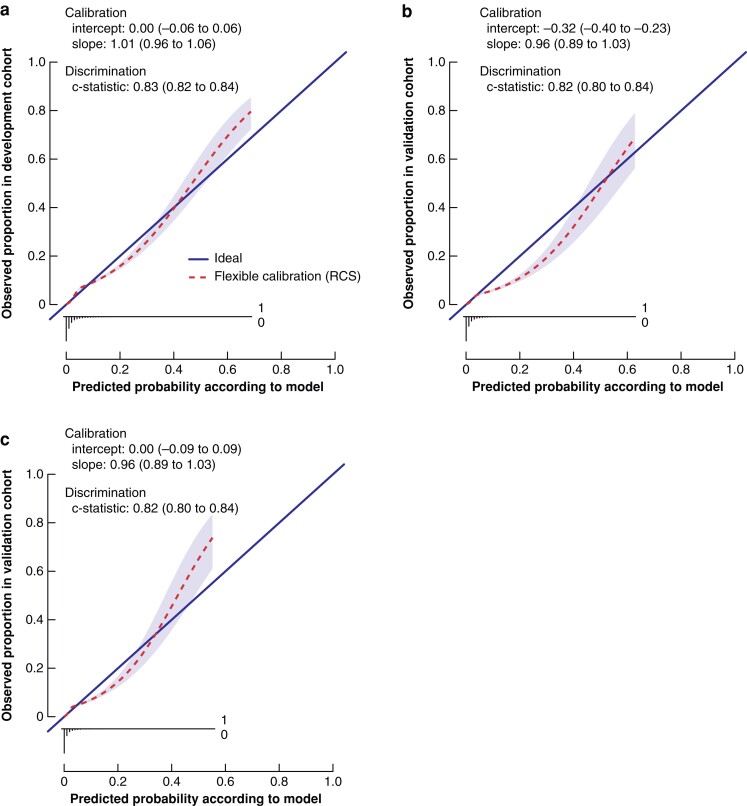
Methods: Data from the Dutch Colorectal Audit were used to assess differences in postoperative outcomes (30-day mortality, hospital stay, blood transfusion, postoperative complications) in patients with CRC treated from 2009 to 2017. Time trends were analysed. Clinical variables were retrieved (including stage, age, sex, BMI, ASA grade, tumour location, timing, surgical approach) and a prediction model with multivariable regression was computed for 30-day mortality using data from 2009 to 2014. The predictive performance of the model was tested among a validation cohort of patients treated between 2015 and 2017.
Results: The prediction model was obtained using data from 51 484 patients and the validation cohort consisted of 32 926 patients. Trends of decreased length of postoperative hospital stay and blood transfusions were found over the years. In stage I-III, postoperative complications declined from 34.3 per cent to 29.0 per cent (P < 0.001) over time, whereas in stage IV complications increased from 35.6 per cent to 39.5 per cent (P = 0.010). Mortality decreased in stage I-III from 3.0 per cent to 1.4 per cent (P < 0.001) and in stage IV from 7.6 per cent to 2.9 per cent (P < 0.001). Eight factors, including stage, age, sex, BMI, ASA grade, tumour location, timing, and surgical approach were included in a 30-day mortality prediction model. The results on the validation cohort documented a concordance C statistic of 0.82 (95 per cent c.i. 0.80 to 0.83) for the prediction model, indicating good discriminative ability.
Conclusion: Postoperative outcome improved in all stages of CRC surgery in the Netherlands. The developed model accurately predicts postoperative mortality risk and is clinically valuable for decision-making.
© The Author(s) 2022. Published by Oxford University Press on behalf of BJS Society Ltd.
Figures
References
-
- Pilleron S, Sarfati D, Janssen-Heijnen M, Vignat J, Ferlay J, Bray Fet al. . Global cancer incidence in older adults, 2012 and 2035: a population-based study. Int J Cancer 2019;144:49–58 - PubMed
-
- Ferlay J, Colombet M, Soerjomataram I, Dyba T, Randi G, Bettio Met al. . Cancer incidence and mortality patterns in Europe: estimates for 40 countries and 25 major cancers in 2018. Eur J Cancer 2018;103:356–387 - PubMed
-
- Iversen LH, Ingeholm P, Gögenur I, Laurberg S. Major reduction in 30-day mortality after elective colorectal cancer surgery: a nationwide population-based study in Denmark 2001–2011. Ann Surg Oncol 2014;21:2267–2273 - PubMed
-
- Kleespies A, Füessl KE, Seeliger H, Eichhorn ME, Müller MH, Rentsch Met al. . Determinants of morbidity and survival after elective non-curative resection of stage IV colon and rectal cancer. Int J Colorectal Dis 2009;24:1097–1109 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
