

Three-port versus four-port technique for laparoscopic cholecystectomy: systematic review and meta-analysis
- PMID: 35357417
- PMCID: PMC8969828
- DOI: 10.1093/bjsopen/zrac013
Three-port versus four-port technique for laparoscopic cholecystectomy: systematic review and meta-analysis
Abstract
Background: The four-port laparoscopic technique is the standard approach for cholecystectomy. A three-port technique has been described, but there is no consensus over the outcomes and efficacy of this approach. The aim was to perform a systematic review and meta-analysis to compare the three- and four-port techniques in laparoscopic cholecystectomy for benign diseases of the gallbladder.
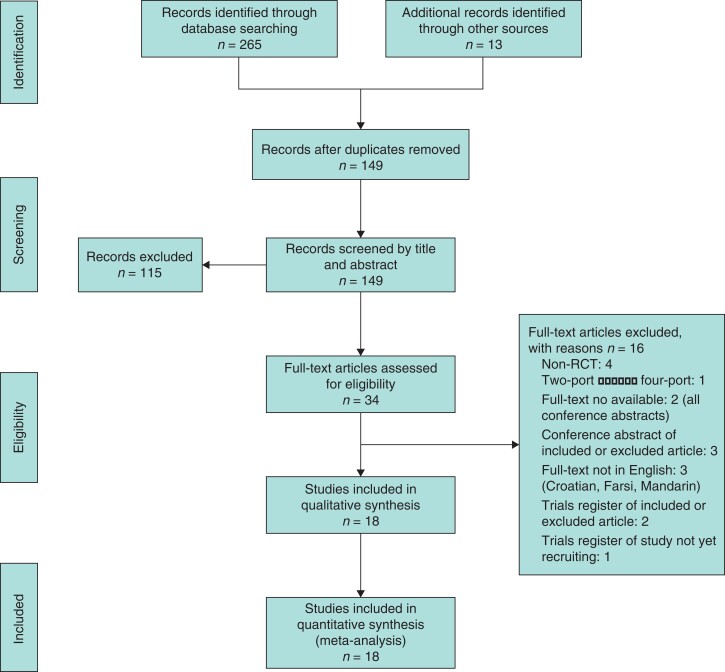
Methods: The review was conducted according to a predefined protocol registered on PROSPERO. Two authors independently conducted an electronic database search of CENTRAL, MEDLINE, Embase, CINAHL, WHO International Clinical Trials Registry, and ClinicalTrials.gov. Outcomes are reported as risk ratios (RR), mean difference (m.d.), or standardized mean difference (s.m.d.) with 95 per cent confidence intervals.
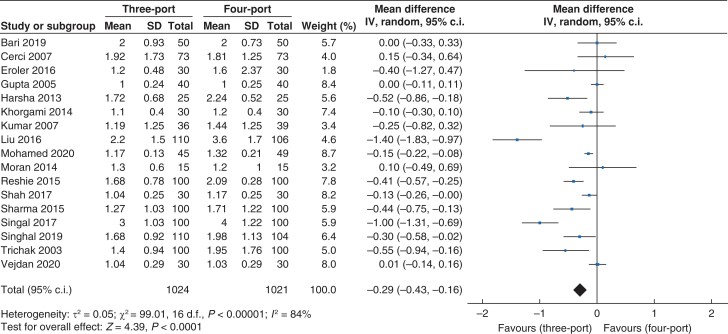
Results: Eighteen trials were included with 2085 patients. Length of hospital stay and postoperative analgesia requirement favoured the three-port group (m.d. -0.29, 95 per cent c.i. -0.43 to -0.16 (P < 0.001); and s.m.d. -0.68, 95 per cent c.i. -1.03 to -0.33 (P < 0.001), respectively). There were no differences in length of procedure or success rate between the two groups (m.d. 0.90, 95 per cent c.i. -3.78 to 5.58 (P = 0.71) and RR 0.99, 95 per cent c.i. 0.97 to 1.01 (P = 0.17), respectively). There were no differences in adverse events. The overall quality of evidence was low.
Conclusion: The three-port technique for laparoscopic cholecystectomy is an option for appropriately trained surgeons who perform it regularly. However, the decision to use three ports should not be at the expense of safe dissection of Calot's triangle.
© The Author(s) 2022. Published by Oxford University Press on behalf of BJS Society Ltd.
Figures










Similar articles
-
Three-Port Laparoscopic Cholecystectomy as a Safe and Feasible Alternative to the Conventional Four-Port Laparoscopic Cholecystectomy.Cureus. 2024 Jan 13;16(1):e52196. doi: 10.7759/cureus.52196. eCollection 2024 Jan. Cureus. 2024. PMID: 38347985 Free PMC article.
-
Port site metastases a year after initial laparoscopic cholecystectomy. Should the use of retrieval bags during laparoscopic cholecystectomy be the new gold standard?Pol Przegl Chir. 2021 May 31;93(6):61-65. doi: 10.5604/01.3001.0015.3280. Pol Przegl Chir. 2021. PMID: 36169533
-
Is the fourth port routinely required for laparoscopic cholecystectomy? Our three-port laparoscopic cholecystectomy experience.Ir J Med Sci. 2016 Nov;185(4):909-912. doi: 10.1007/s11845-016-1493-8. Epub 2016 Aug 31. Ir J Med Sci. 2016. PMID: 27582090
-
Three-dimensional versus two-dimensional imaging during laparoscopic cholecystectomy: a systematic review and meta-analysis of randomised controlled trials.Langenbecks Arch Surg. 2020 Aug;405(5):563-572. doi: 10.1007/s00423-020-01909-9. Epub 2020 Jun 22. Langenbecks Arch Surg. 2020. PMID: 32572555
-
Retrieval of Gallbladder Via Umbilical Versus Epigastric Port Site During Laparoscopic Cholecystectomy: A Systematic Review and Meta-Analysis.Surg Laparosc Endosc Percutan Tech. 2019 Oct;29(5):321-327. doi: 10.1097/SLE.0000000000000662. Surg Laparosc Endosc Percutan Tech. 2019. PMID: 31033631
Cited by
-
Systematic Review of Utilized Ports in Laparoscopic Cholecystectomy: Pushing the Boundaries.Minim Invasive Surg. 2024 May 23;2024:9961528. doi: 10.1155/2024/9961528. eCollection 2024. Minim Invasive Surg. 2024. PMID: 38826773 Free PMC article. Review.
-
Avoidance of bile duct injury in laparoscopic cholecystectomy with feasible intraoperative resources: A cohort study.Biomed Rep. 2024 Jun 5;21(2):110. doi: 10.3892/br.2024.1798. eCollection 2024 Aug. Biomed Rep. 2024. PMID: 38872852 Free PMC article.
-
Comparison of modified thoracoabdominal nerve block through perichondral approach and subcostal transversus abdominis plane block for pain management in laparoscopic cholecystectomy: a randomized-controlled trial.Korean J Pain. 2023 Jul 1;36(3):382-391. doi: 10.3344/kjp.23114. Epub 2023 Jun 20. Korean J Pain. 2023. PMID: 37336756 Free PMC article.
-
Machine learning algorithms as early diagnostic tools for prolonged operative time in patients with fluorescent laparoscopic cholecystectomy: a retrospective cohort study.Front Surg. 2025 Jun 23;12:1582425. doi: 10.3389/fsurg.2025.1582425. eCollection 2025. Front Surg. 2025. PMID: 40625676 Free PMC article.
-
Comparative study of three-port vs four-port laparoscopic cholecystectomy in a cohort study: a surgical task load survey.Updates Surg. 2025 Jul 4. doi: 10.1007/s13304-025-02308-9. Online ahead of print. Updates Surg. 2025. PMID: 40614033
References
-
- Association of Upper Gastrointestinal Surgeons (AUGIS) . Commissioning Guide: Gallstone Disease. https://www.augis.org/Guidelines/AUGIS-Guidelines (accessed 9 January 2022)
-
- Royal College of Surgeons of England (RCSEng) and Association of Surgeons of Great Britain and Ireland (ASGBI) . Commissioning Guide: Emergency General Surgery (Acute Abdominal Pain). https://www.rcseng.ac.uk/library-and-publications/rcs-publications/docs/... (accessed 9 January 2022)
-
- NIH Consensus Development Panel on Gallstones and Laparoscopic Cholecystectomy. JAMA 1993;269:1018–1024 - PubMed
-
- Tagaya N, Kita J, Takagi K, Imada T, Ishikawa K, Kogure H et al. Experience with three-port laparoscopic cholecystectomy. J Hepatobiliary Pancreat Surg 1998;5:309–311 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
