

Effectiveness of sequential biologic and targeted disease modifying anti-rheumatic drugs for rheumatoid arthritis
- PMID: 35357421
- PMCID: PMC9707051
- DOI: 10.1093/rheumatology/keac190
Effectiveness of sequential biologic and targeted disease modifying anti-rheumatic drugs for rheumatoid arthritis
Abstract
Objectives: Whether patients with RA benefit from repeated trials of biologic or targeted synthetic DMARDs (b/tsDMARDs) after three or more attempts is unknown. We aimed to describe treatment outcomes in each line of b/tsDMARD therapy.
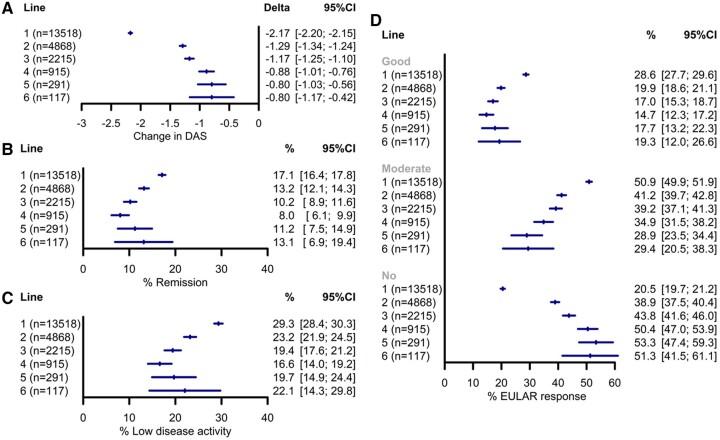
Methods: Using data from the British Society for Rheumatology Biologics Register for RA from 2001 to 2020, change to a new b/tsDMARD (except biosimilar switches) was defined as a new line of therapy. Treatment outcomes were compared across lines of therapy, including DAS28 remission (≤2.6), low disease activity (LDA, ≤3.2) at 6 months and median time to drug discontinuation. Multiple imputation was used for missing data.
Results: A total of 22 934 individuals starting a first b/tsDMARD were included (mean age 56 years, 76% female), among whom 10 823 commenced a second-line drug, 5056 third, 2128 fourth, 767 fifth and 292 sixth. Most (71%) had sufficient data for DAS28-derived outcome analyses. TNF inhibitors were the most common first-line drug, but choice of subsequent-line drugs changed over time. Seventeen percent achieved DAS28 remission following first-line, 13% second and 8-13% with third through sixth. LDA was achieved in 29% of first-line, 23% second, 17-22% through to the sixth. Patients stayed on first-line therapy for a median of 2.6 years, ranging from 1.0-1.4 years for lines two to six.
Conclusion: Many patients will eventually benefit after repeated trials of b/tsDMARD. Further research to improve treatment selection are needed to prevent prolonged trial and error approaches in some patients.
Keywords: DMARDs; RA; biologics; difficult to treat; effectiveness; switching.
© The Author(s) 2022. Published by Oxford University Press on behalf of the British Society for Rheumatology.
Figures



References
-
- Hyrich KL, Watson KD, Lunt M, Symmons DPM, on behalf of the British Society for Rheumatology Biologics Register (BSRBR). Changes in disease characteristics and response rates among patients in the United Kingdom starting anti-tumour necrosis factor therapy for rheumatoid arthritis between 2001 and 2008. Rheumatology (Oxford) 2011;50:117–23. - PMC - PubMed
-
- de Hair MJH, Jacobs JWG, Schoneveld JLM, van Laar JM.. Difficult-to-treat rheumatoid arthritis: an area of unmet clinical need. Rheumatology (Oxford) 2018;57:1135–44. - PubMed
-
- Roodenrijs NMT, van der Goes MC, Welsing PMJ. et al. Difficult-to-treat rheumatoid arthritis: contributing factors and burden of disease. Rheumatology (Oxford) 2021;60:3778–88. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
