

Likelihood of Lung Cancer Screening by Poor Health Status and Race and Ethnicity in US Adults, 2017 to 2020
- PMID: 35357450
- PMCID: PMC8972038
- DOI: 10.1001/jamanetworkopen.2022.5318
Likelihood of Lung Cancer Screening by Poor Health Status and Race and Ethnicity in US Adults, 2017 to 2020
Erratum in
-
Errors in Abstract, Introduction, and Methods.JAMA Netw Open. 2022 May 2;5(5):e2213694. doi: 10.1001/jamanetworkopen.2022.13694. JAMA Netw Open. 2022. PMID: 35522288 Free PMC article. No abstract available.
Abstract
Importance: Lung cancer screening (LCS) via low-dose chest computed tomography can prevent mortality through surgical resection of early-stage cancers, but it is unknown whether poor health is associated with screening. Though LCS may be associated with better outcomes for non-Hispanic Black individuals, it is unknown whether racial or ethnic disparities exist in LCS use.
Objective: To determine whether health status is associated with LCS and whether racial or ethnic disparities are associated with LCS independently of health status.
Design, setting, and participants: This cross-sectional, population-based study of community-dwelling US adults used data from Behavioral Risk Factor Surveillance System annual surveys, 2017 to 2020. Participants were aged 55 to 79 years, with a less than 30 pack-year smoking history, and were current smokers or those who quit within 15 years. Data were analyzed from August to November 2021.
Exposures: Self-reported health status and race and ethnicity.
Main outcomes and measures: Self-reported LCS in the last 12 months.
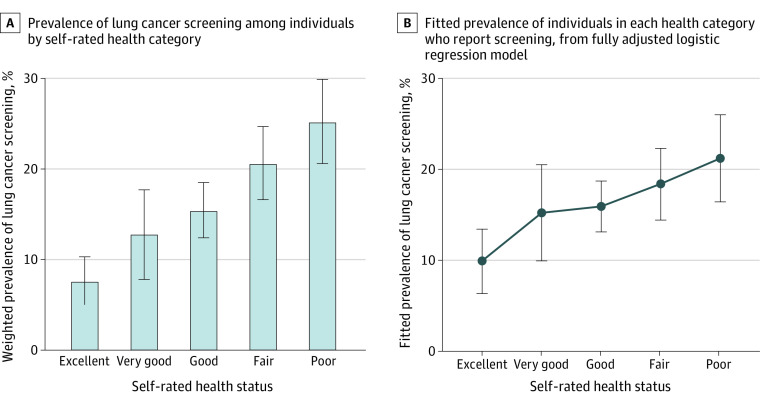
Results: Of 14 550 individuals (7802 men [55.5%]; 7527 [55.0%] aged 65-79 years [percentages are weighted]), representing 3.68 million US residents, 17.0% (95% CI, 15.1%-18.9%) reported undergoing LCS. The prevalence of LCS was lower among non-Hispanic Black than non-Hispanic White individuals but not to a significant degree (12.0% [95% CI, 4.3%-19.7%] vs 17.5% [95% CI, 15.6%-19.5%]; P = .57). Health status was associated with LCS: 468 individuals in poor health vs 96 individuals in excellent health reported LCS (25.2% [95% CI, 20.6%-29.9%] vs 7.6% [95% CI, 5.0%-10.3%]; P < .001), and those with difficulty climbing stairs were more likely to report LCS than those without this functional limitation. Adjusting for sociodemographic factors, functional status, and comorbidities, self-rated health status remained associated with LCS (adjusted odds ratio, 1.19 per each 1-step decline in health; 95% CI, 1.03-1.38), and non-Hispanic Black individuals were 53% less likely to report LCS than non-Hispanic White individuals (adjusted odds ratio, 0.47; 95% CI, 0.24-0.90). Results were robust in sensitivity analyses in which health was alternatively quantified as number of comorbidities.
Conclusions and relevance: LCS in the US is more common among those who may be less likely to benefit from screening because of poor underlying health. Furthermore, racial or ethnic disparities were evident after accounting for health status, with non-Hispanic Black individuals nearly half as likely as non-Hispanic White individuals to report LCS despite the potential for greater benefit of screening this population.
Conflict of interest statement
Figures
References
-
- Howlader N, Noone AM, Krapcho M, et al. , eds. SEER cancer statistics review, 1975-2018. National Cancer Institute. April 15, 2021. Accessed August 9, 2021. https://seer.cancer.gov/csr/1975_2018/
-
- Jonas D, Reuland D, Reddy S, et al. Screening for lung cancer with low-dose computed tomography: an evidence review for the U.S. Preventive Services Task Force. March 9, 2021. Accessed September 7, 2021. https://www.uspreventiveservicestaskforce.org/uspstf/document/final-evid... - PubMed
