

Off-Label Use of Tenecteplase for the Treatment of Acute Ischemic Stroke: A Systematic Review and Meta-analysis
- PMID: 35357458
- PMCID: PMC8972028
- DOI: 10.1001/jamanetworkopen.2022.4506
Off-Label Use of Tenecteplase for the Treatment of Acute Ischemic Stroke: A Systematic Review and Meta-analysis
Abstract
Importance: Tenecteplase is being evaluated as an alternative thrombolytic agent for the treatment of acute ischemic stroke (AIS) within ongoing randomized clinical trials (RCTs). In addition, nonrandomized clinical experiences with off-label use of tenecteplase vs alteplase for AIS treatment are being published.
Objective: To evaluate the available evidence on the safety and efficacy of intravenous tenecteplase compared with intravenous alteplase provided by nonrandomized studies.
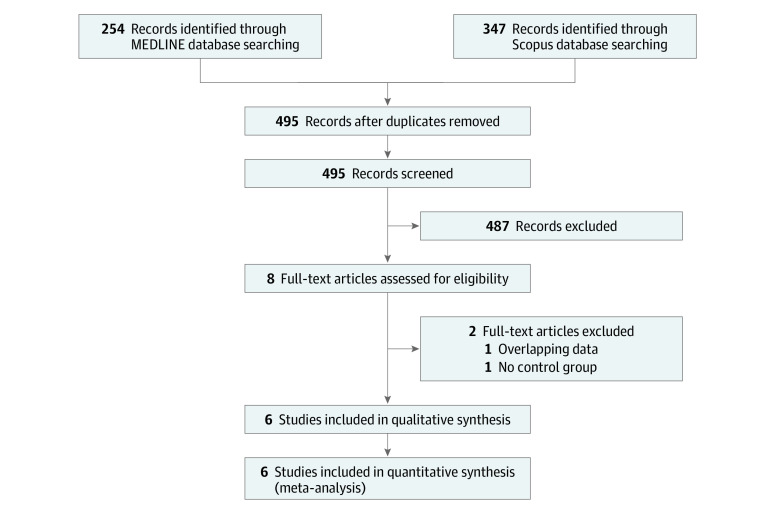
Data sources: Eligible studies were identified by searching MEDLINE and Scopus databases. No language or other restrictions were imposed. The literature search was conducted on October 12, 2021. This meta-analysis used the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and was written according to the Meta-analysis of Observational Studies in Epidemiology (MOOSE) proposal.
Study selection: Nonrandomized studies (prospective or retrospective) comparing intravenous tenecteplase (at any dose) with intravenous alteplase in patients with AIS were included in the analysis.
Data extraction and synthesis: The crude odds ratios (ORs) and 95% CIs were calculated for the association of tenecteplase vs alteplase with the outcomes of interest and adjusted ORs were extracted if provided. Estimates using random-effects models were pooled.
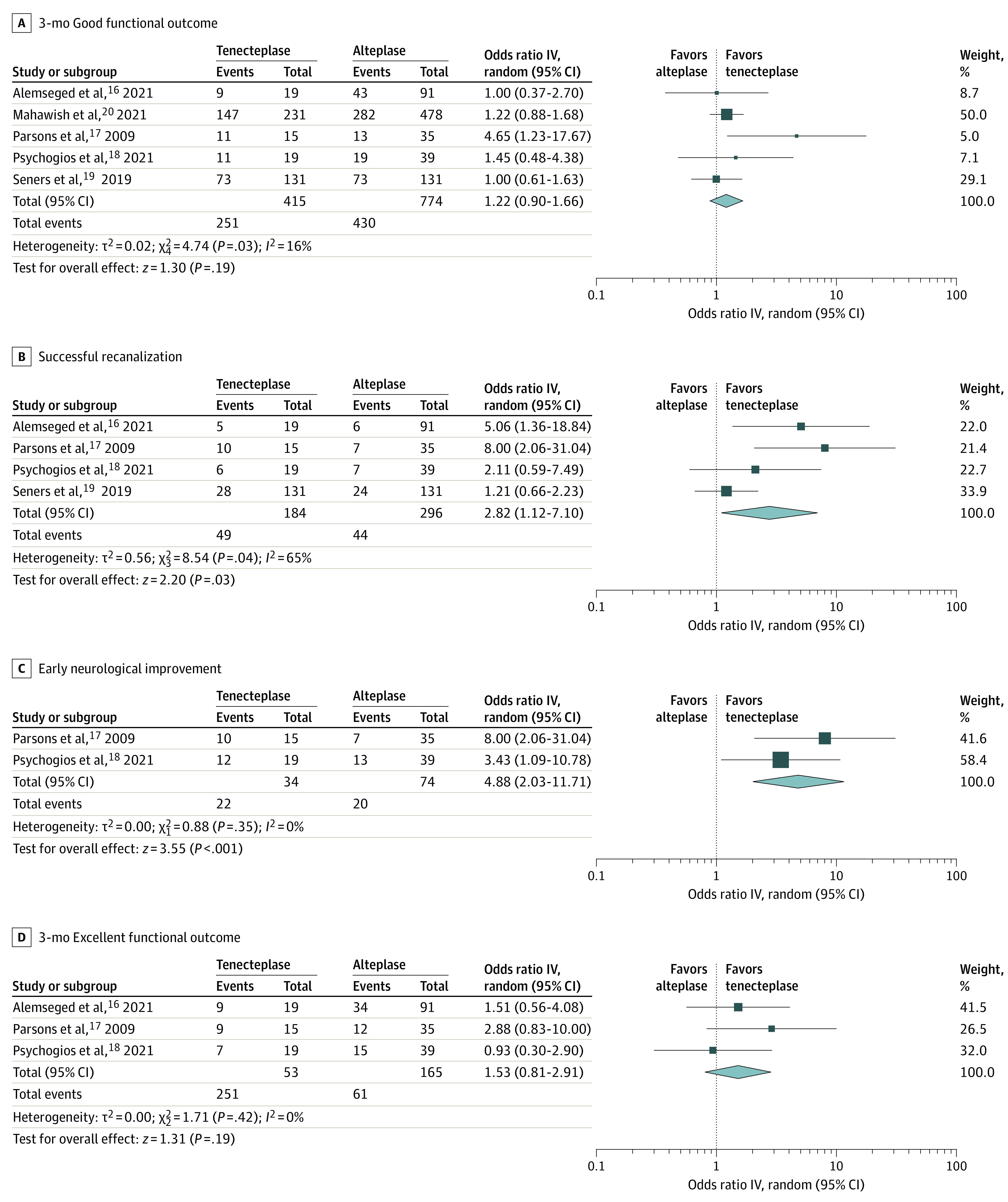
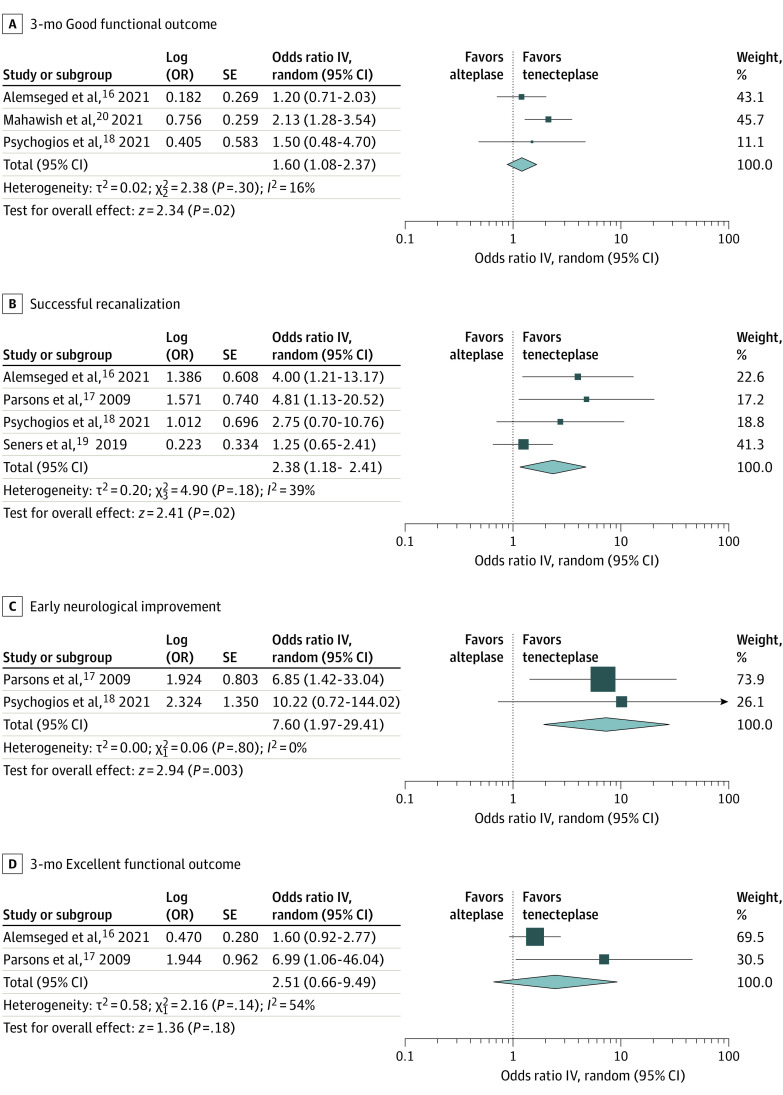
Main outcomes and measures: The primary outcome was the probability of good functional outcome (modified Rankin scale [mRS] score, 0-2) at 90 days.
Results: Six studies were identified including a total of 1820 patients (618 [34%] treated with tenecteplase). Patients receiving tenecteplase had higher odds of 3-month good functional outcome (crude odds ratio [OR], 1.22; 95% CI, 0.90-1.66; adjusted OR, 1.60, 95% CI, 1.08-2.37), successful recanalization (crude OR, 2.82; 95% CI, 1.12-7.10; adjusted OR, 2.38; 95% CI, 1.18-4.81), and early neurological improvement (crude OR, 4.88; 95% CI, 2.03-11.71; adjusted OR, 7.60; 95% CI, 1.97-29.41). No significant differences were detected in 3-month excellent functional outcome proportions (mRS score 0-1; crude OR, 1.53; 95% CI, 0.81-2.91; adjusted OR, 2.51; 95% CI, 0.66- 9.49), symptomatic intracranial hemorrhage (crude OR, 0.97; 95% CI, 0.44-2.16; adjusted OR, 1.16; 95% CI, 0.13-10.50), or parenchymal hematoma (crude OR, 1.20; 95% CI, 0.24-5.95).
Conclusions and relevance: Evidence from nonrandomized studies suggests tenecteplase is as safe as alteplase and potentially associated with improved functional outcomes compared with alteplase. Based on these findings, enrollment in the ongoing RCTs appears to be appropriate.
Conflict of interest statement
Figures
References
-
- Stroke Foundation . Clinical guidelines for stroke management (2021). Accessed October 12, 2021. https://informme.org.au/guidelines/clinical-guidelines-for-stroke-manage...
