

Efficiency of Electronic Health Record Assessment of Patient-Reported Outcomes After Cancer Immunotherapy: A Randomized Clinical Trial
- PMID: 35357459
- PMCID: PMC8972037
- DOI: 10.1001/jamanetworkopen.2022.4427
Efficiency of Electronic Health Record Assessment of Patient-Reported Outcomes After Cancer Immunotherapy: A Randomized Clinical Trial
Abstract
Importance: Cancer immunotherapy causes a wide range of immune-related adverse events (irAEs) that require close and timely follow-up.
Objectives: To compare the efficiency between electronic patient-reported outcomes (ePRO) and traditional follow-up models in cancer immunotherapy.
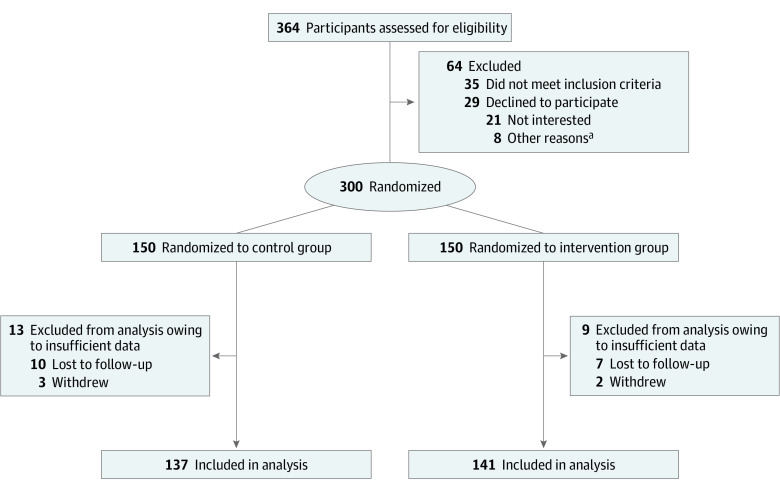
Design, setting, and participants: This open-label randomized clinical trial was performed from September 1, 2019, to March 31, 2021. Patients were randomized to the ePRO model intervention or a control group by a computer system. A total of 28 Chinese tertiary care hospitals participated. Patients who were receiving cancer immunotherapy and could use smartphones or computers were eligible. A total of 300 patients were screened and 278 (92.7%) were enrolled.
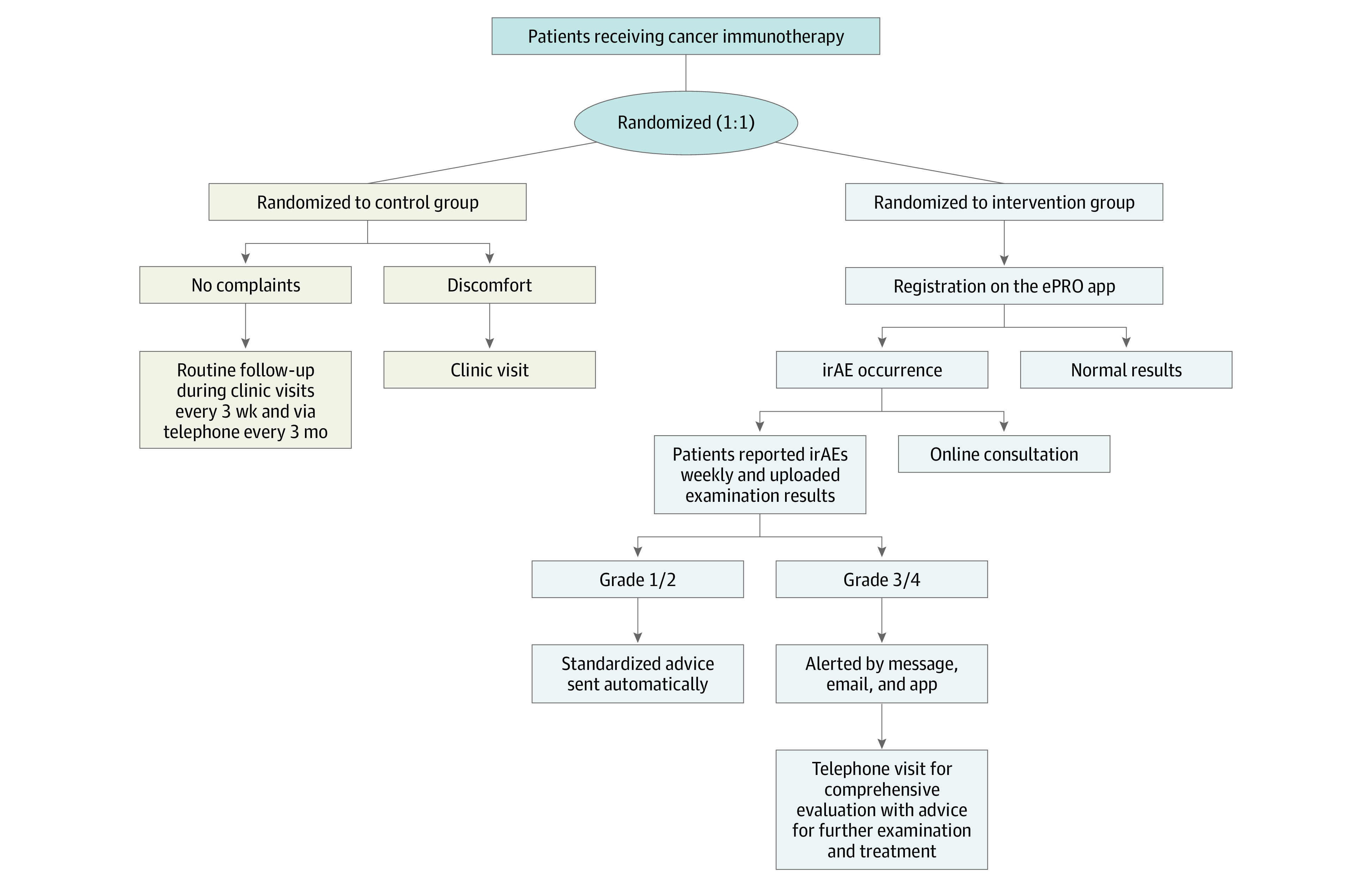
Interventions: The control group was followed up using traditional methods, including clinic visits every 21 days and telephone follow-up every 3 months. In the intervention group, the ePRO follow-up model included a questionnaire of common symptoms and an image recognition function to evaluate grades of typical irAEs. Patients completed questionnaires weekly and uploaded pictures of results between visits. When grade 1 or 2 irAEs occurred, standardized advice was sent automatically. If grade 3 or 4 irAEs were reported, the model alerted the health care team for assessment and intervention immediately. All patients were followed up for 6 months or until treatment completion.
Main outcomes and measures: Incidence of serious (grades 3 to 4) irAEs, emergency department (ED) visits, quality of life (QOL), time spent implementing the ePRO model, rate of treatment discontinuation, and death were compared between groups post intervention.
Results: A total of 278 patients (mean [SD] age, 58.8 [12.7 (range, 27-78)] years; 206 men [74.1%]) were included in the analysis, consisting of 141 in the intervention group and 137 in the control group. At the postintervention evaluation, the intervention group showed a reduced incidence of serious irAEs (29 of 141 [20.6%] vs 46 of 137 [33.6%]; hazard ratio [HR], 0.51 [95% CI, 0.30-0.88]; P = .01), fewer ED visits (23 of 141 [16.3%] vs 41 of 137 [29.9%]; HR, 0.46 [95% CI, 0.26-0.81]; P = .01), a lower rate of treatment discontinuation (5 of 141 [3.6%] vs 15 of 137 [11.0%]; HR, 0.30 [95% CI, 0.11-0.85]; P = .02), a higher QOL level (mean [SD] score, 74.2 [15.1; 95% CI, 71.7-76.9] vs 64.7 [28.5; 95% CI, 61.0-68.4]; P = .001), and less time implementing follow-up (mean [SD], 8.2 [3.9; 95% CI, 5.0-10.6] minutes vs 36.1 [15.3; 95% CI, 33.6-38.8] minutes; P < .001). However, there were no significant differences between groups in death rates (2 of 141 [1.4%] vs 5 of 137 [3.6%]; HR, 0.38 [95% CI, 0.07-1.99]; P = .28).
Conclusions and relevance: This randomized clinical trial found that the ePRO follow-up model can improve safety and QOL of patients receiving cancer immunotherapy as well as reduce time spent monitoring. This model may provide reliable information and management recommendations.
Trial registration: Chinese Clinical Trial Registry Identifier: ChiCTR2100052819.
Conflict of interest statement
Figures
Comment in
-
An Assistive Electronic Patient-Reported Outcome Monitoring Intervention for Management of Immune-Related Toxic Effects-Moving Toward Efficiency and Scale.JAMA Netw Open. 2022 Mar 1;5(3):e224437. doi: 10.1001/jamanetworkopen.2022.4437. JAMA Netw Open. 2022. PMID: 35357462 Free PMC article. No abstract available.
References
-
- Brahmer JR, Lacchetti C, Schneider BJ, et al. ; National Comprehensive Cancer Network . Management of immune-related adverse events in patients treated with immune checkpoint inhibitor therapy: American Society of Clinical Oncology clinical practice guideline. J Clin Oncol. 2018;36(17):1714-1768. doi: 10.1200/JCO.2017.77.6385 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
