

Editorial
doi: 10.1182/blood.2021015340.
Pulmonary hypertension in thalassemia: a call to action
Affiliations
- PMID: 35357479
- PMCID: PMC8972095
- DOI: 10.1182/blood.2021015340
Item in Clipboard
Editorial
Pulmonary hypertension in thalassemia: a call to action
Blood.
.
No abstract available
Conflict of interest statement
Conflict-of-interest disclosure: J.C.W. consults for Celgene, WorldCareClinical, ImagoBiosciences, and Silence Therapeutics. He receives research support from the National Institutes of Health (NIH), Philips Medical Systems, the Saban Research Institute, and the Additional Ventures Single Ventricle Fund.
Figures
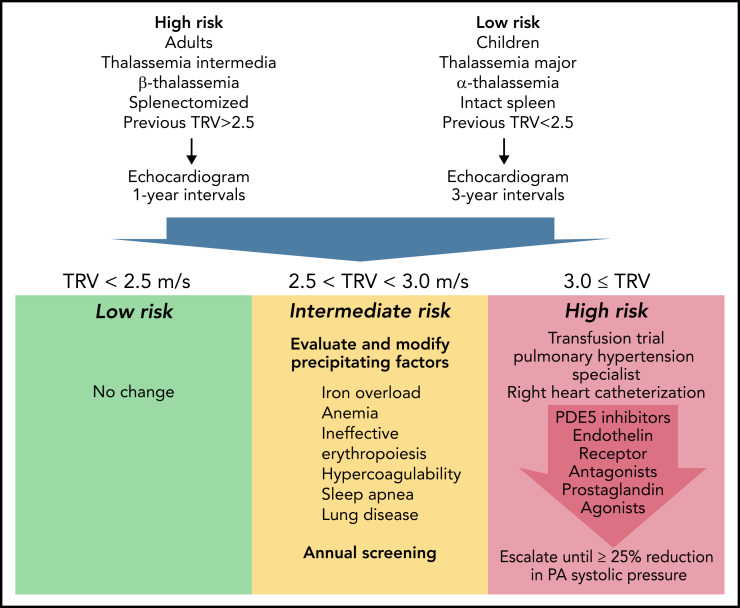
Proposed Algorithm For Screening and Treatment of Pulmonary Hypertension in Thalassemia. Represents candidate pulmonary arterial hypertension guidelines informed by the WebThal data. The risk of pulmonary hypertension increases with age and splenectomy, as well as the severity of anemia and ineffective erythropoiesis (which is impacted by genotype). The frequency of echocardiogram screening should reflect these apriori risks, as well as previous echocardiogram results. TRV results <2.5 meters per second are normal and require no change in monitoring or therapy. TRV results between 2.5 and 2.9 meters per second indicate an abnormal physiology that could potentially progress to pulmonary arterial hypertension. The hematologist must carefully examine potential underlying factors and try to ameliorate them, using serial TRV assessment as the biomarker of success. Regardless of apriori pulmonary hypertension risk, a documented abnormal TRV above 2.5 meters per second suggests a high-risk phenotype and annual follow-up. A TRV of 3.0 meters per second or higher demarcates a patient at significant risk for catheter-proven pulmonary artery hypertension. A first, critical, step is initiation or intensification of chronic transfusion therapy to completely suppress endogenous erythropoiesis. In early disease, this can be sufficient to normalize pulmonary artery pressures. If unsuccessful, the patient should be referred to a pulmonary hypertension specialist for right heart catheterization and aggressive titration of pulmonary hypertension therapies to a target goal of 25% reduction in pulmonary artery systolic pressure.
Comment on
-
Mortality in β-thalassemia patients with confirmed pulmonary arterial hypertension on right heart catheterization.Blood. 2022 Mar 31;139(13):2080-2083. doi: 10.1182/blood.2021014862. Blood. 2022. PMID: 34986266 No abstract available.
References
-
- Pinto VM, Musallam KM, Derchi GE, et al. . Mortality in β-thalassemia patients with confirmed pulmonary arterial hypertension on right heart catheterization. Blood. 2022; 139(13):2080-2083. - PubMed
-
- Derchi G, Galanello R, Bina P, et al. ; Webthal Pulmonary Arterial Hypertension Group* . Prevalence and risk factors for pulmonary arterial hypertension in a large group of β-thalassemia patients using right heart catheterization: a Webthal study. Circulation. 2014;129(3):338-345. - PubMed
-
- Klinger JR, Elliott CG, Levine DJ, et al. . Therapy for pulmonary arterial hypertension in adults: update of the CHEST guideline and expert panel report [published correction appears in Chest. 2021;159(1):457]. Chest. 2019;155(3):565-586. - PubMed
-
- Teawtrakul N, Ungprasert P, Pussadhamma B, et al. . Effect of genotype on pulmonary hypertension risk in patients with thalassemia. Eur J Haematol. 2014;92(5):429-434. - PubMed
-
- Aessopos A, Farmakis D, Hatziliami A, et al. . Cardiac status in well-treated patients with thalassemia major. Eur J Haematol. 2004; 73(5):359-366. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
