

Long-term Outcomes Following Esophagectomy in Older and Younger Adults with Esophageal Cancer
- PMID: 35357674
- PMCID: PMC9474270
- DOI: 10.1007/s11605-022-05295-z
Long-term Outcomes Following Esophagectomy in Older and Younger Adults with Esophageal Cancer
Abstract
Background: Patterns of overall and disease-free survival after esophagectomy for esophageal cancer in older adults have not been carefully studied.
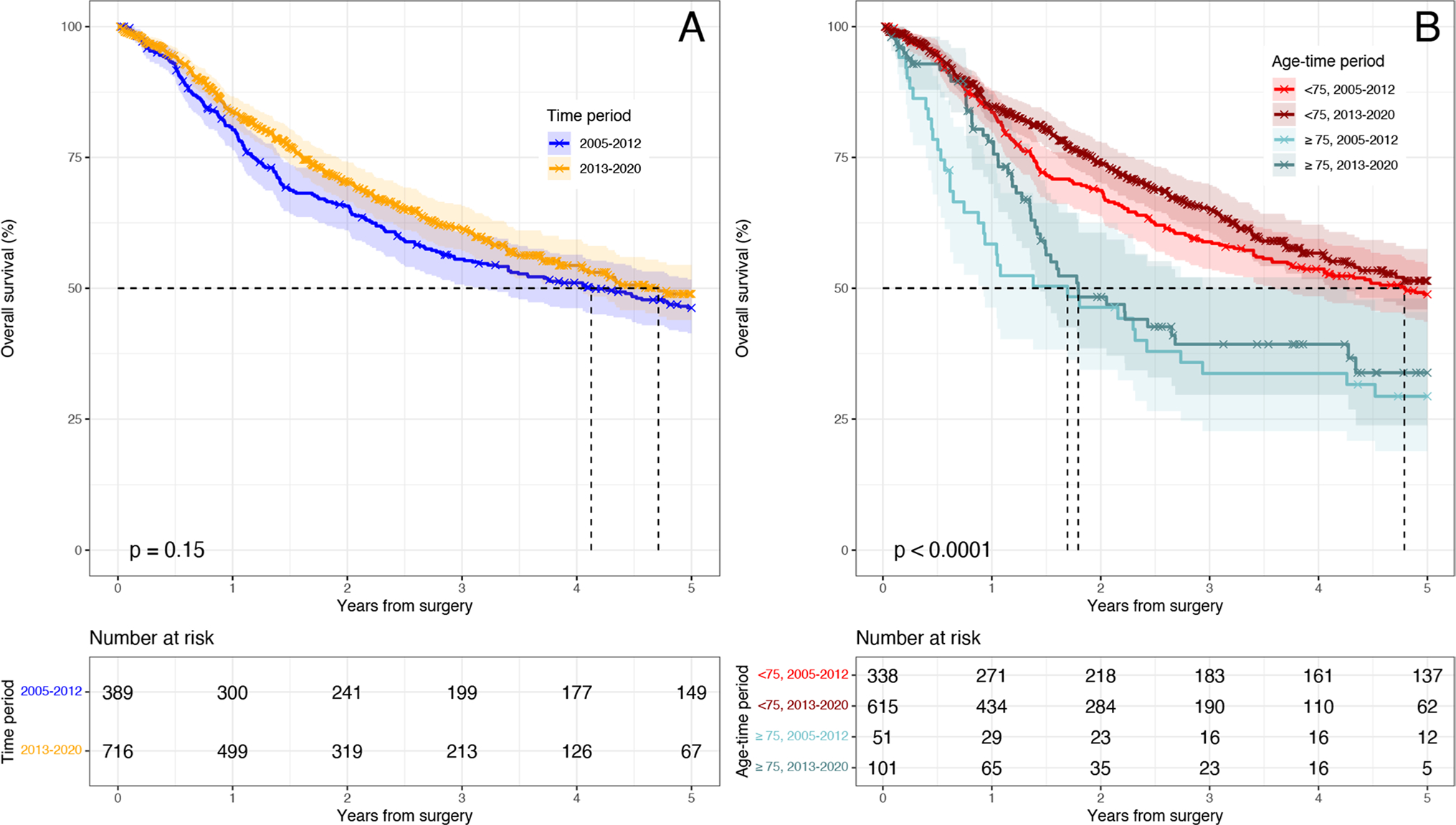
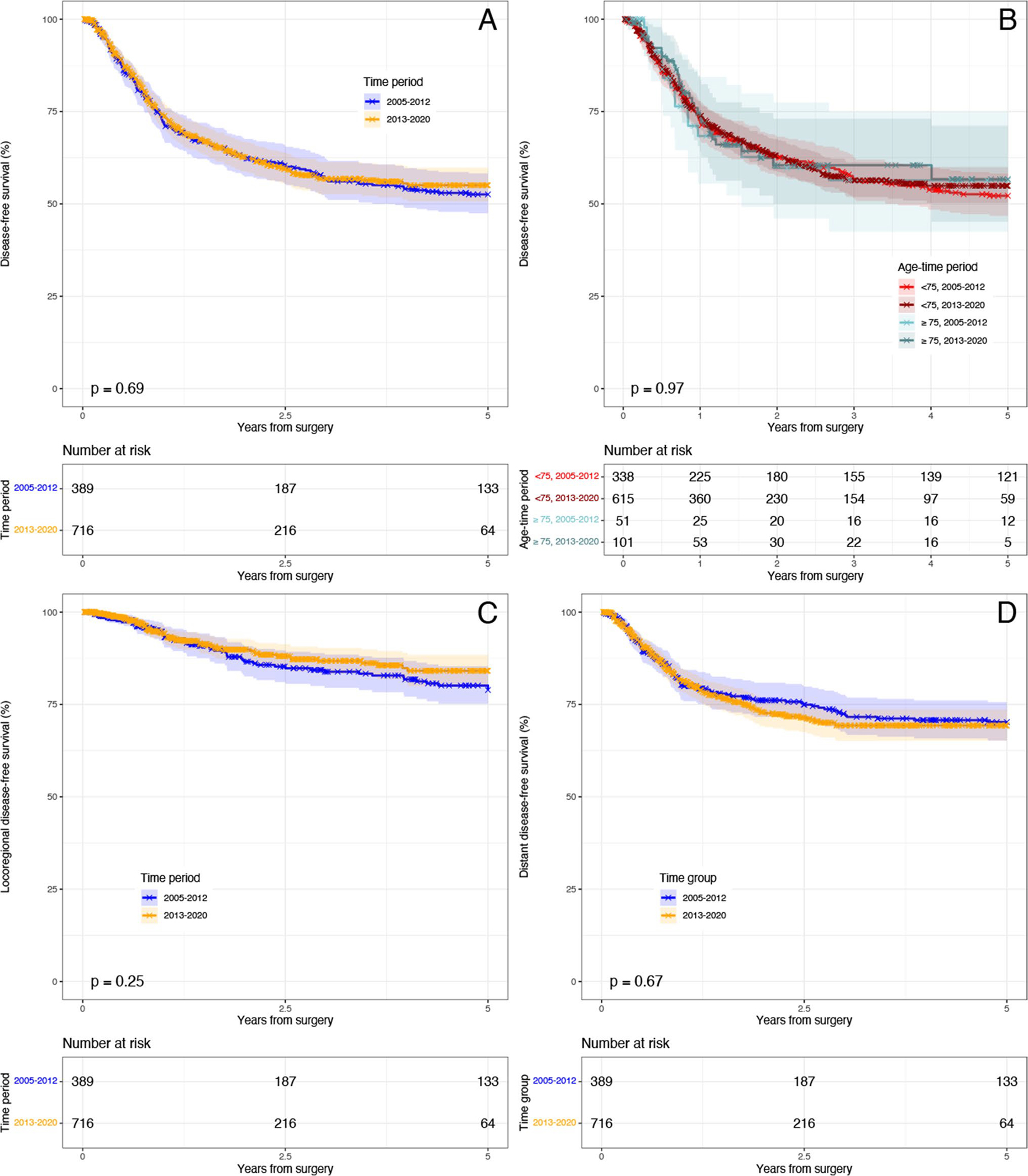
Methods: Retrospective analysis of all patients with esophageal cancer undergoing esophagectomy from 2005 to 2020 at our institution was performed. Differences in outcomes were stratified by age groups, < 75 and ≥ 75 years old, and two time periods, 2005-2012 and 2013-2020.
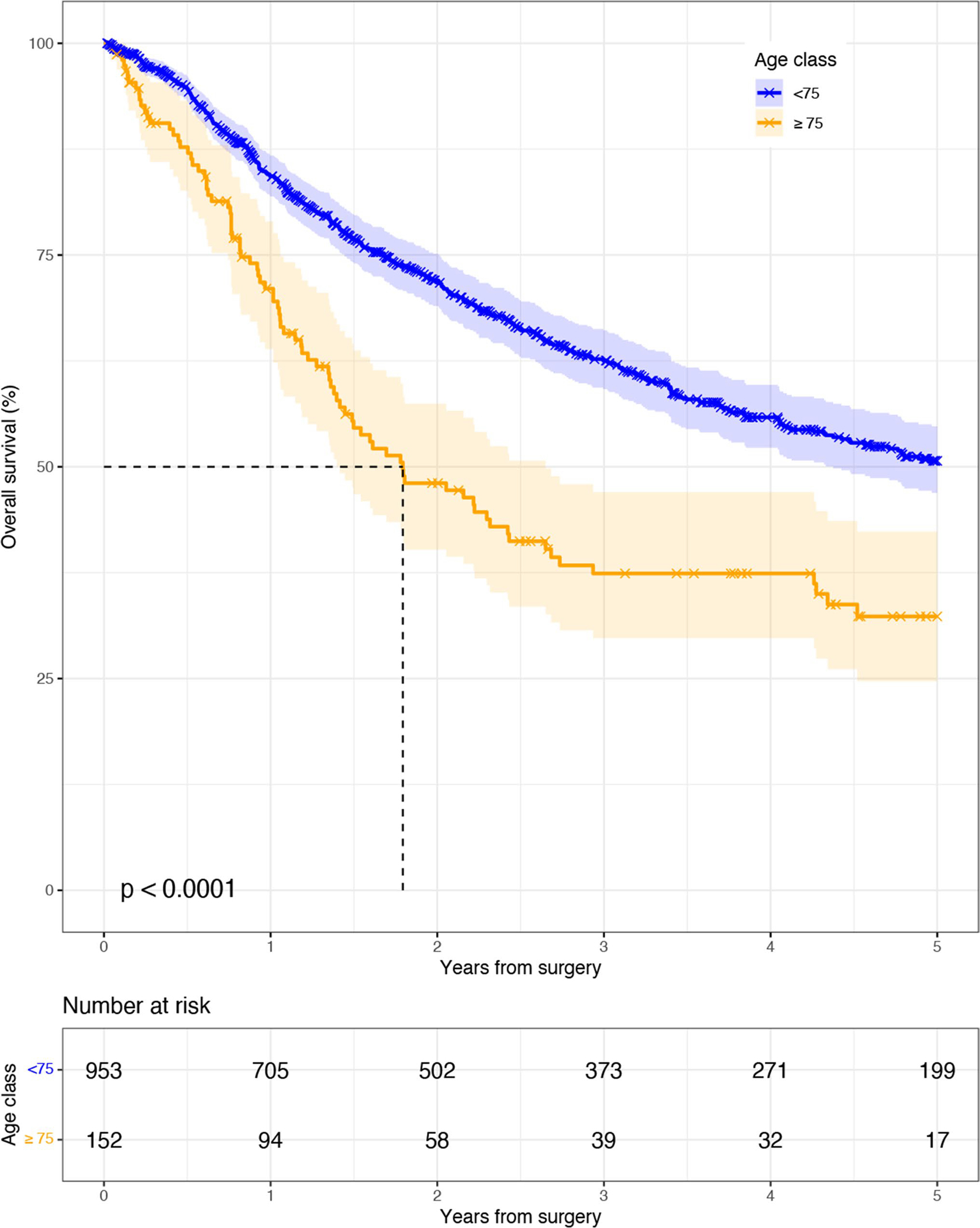
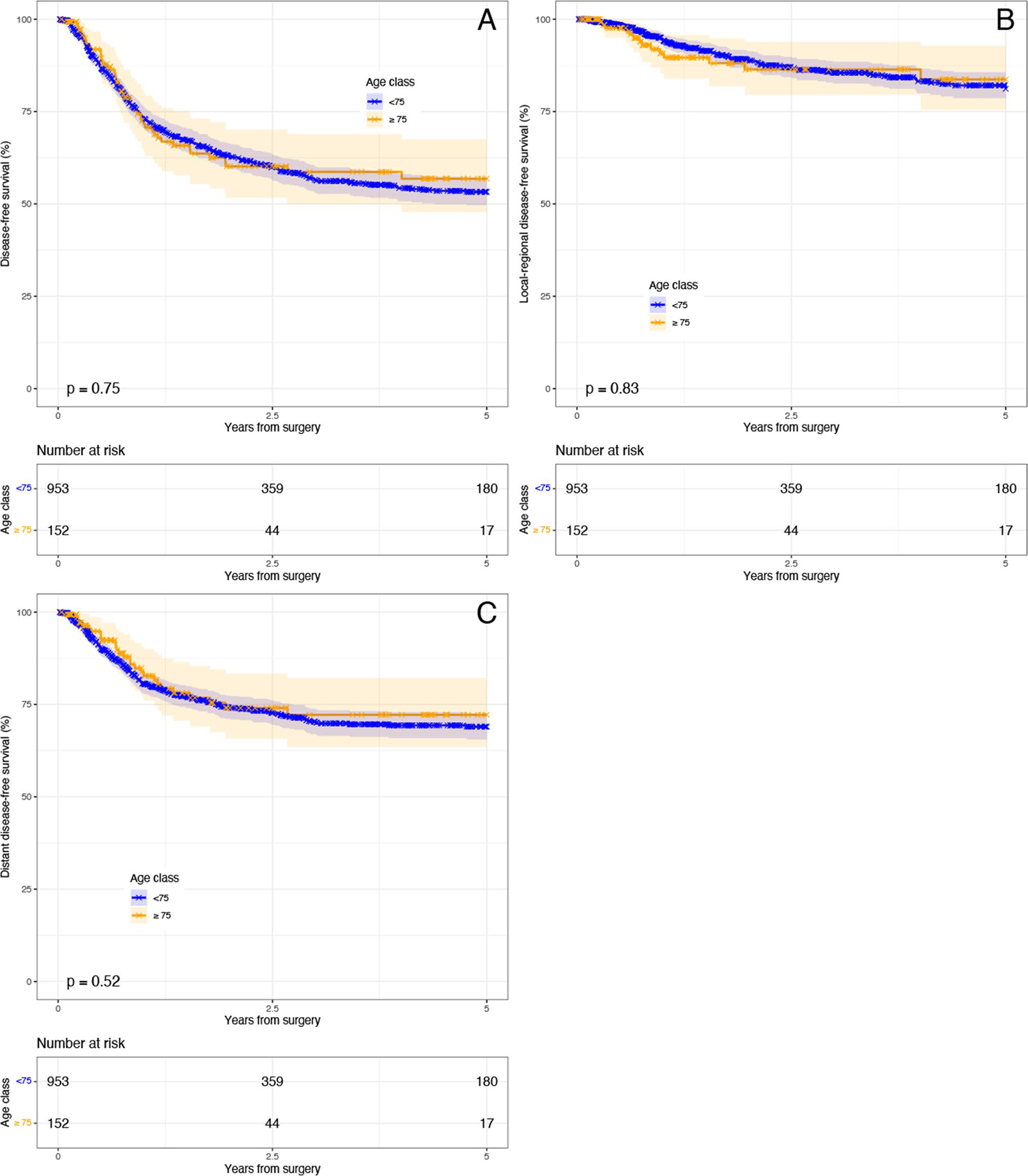
Results: A total of 1135 patients were included: 979 (86.3%) patients were < 75 (86.3%), and 156 (13.7%) were ≥ 75 years old. Younger patients had fewer comorbidities, better nutritional status, and were more likely to receive neoadjuvant and adjuvant therapy (all p < 0.05). However, tumor stage and operative approach were similar, except for increased performance of the McKeown technique in younger patients (p = 0.02). Perioperatively, younger patients experienced fewer overall and grade II complications (both p < 0.05). They had better overall survival (log-rank p-value < 0.001) and median survival, 62.2 vs. 21.5 months (p < 0.05). When stratified by pathologic stage, survival was similar for yp0 and pathologic stage II disease (both log-rank p-value > 0.05). Multivariable Cox models showed older age (≥ 75 years old) had increased hazard for reduced overall survival (HR 2.04 95% CI 1.5-2.8; p < 0.001) but not disease-free survival (HR 1.1 95% CI 0.78-1.6; p = 0.54). Over time, baseline characteristics remained largely similar, while stage became more advanced with a rise in neoadjuvant use and increased performance of minimally invasive esophagectomy (all p < 0.05). While overall complication rates improved (p < 0.05), overall and recurrence-free survival did not. Overall survival was better in younger patients during both time periods (both log-rank p < 0.05).
Conclusions: Despite similar disease-free survival rates, long-term survival was decreased in older adults as compared to younger patients. This may be related to unmeasured factors including frailty, long-term complications after surgery, and competing causes of death. However, our results suggest that survival is similar in those with complete pathologic responses.
Keywords: Esophagectomy; Older adults; Outcomes; Recurrence; Survival.
© 2022. The Society for Surgery of the Alimentary Tract.
Conflict of interest statement
Declarations
Figures
References
-
- Cancer of the Esophagus - Cancer Stat Facts. SEER, https://seer.cancer.gov/statfacts/html/esoph.html (accessed 13 May 2020).
-
- Cijs TM, Verhoef C, Steyerberg EW, et al. Outcome of esophagectomy for cancer in elderly patients. Ann Thorac Surg 2010; 90: 900–907. - PubMed
-
- Schlottmann F, Strassle PD, Nayyar A, et al. Postoperative outcomes of esophagectomy for cancer in elderly patients. Journal of Surgical Research 2018; 229: 9–14. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
