

Suppression of human and simian immunodeficiency virus replication with the CCR5-specific antibody Leronlimab in two species
- PMID: 35358290
- PMCID: PMC8970399
- DOI: 10.1371/journal.ppat.1010396
Suppression of human and simian immunodeficiency virus replication with the CCR5-specific antibody Leronlimab in two species
Abstract
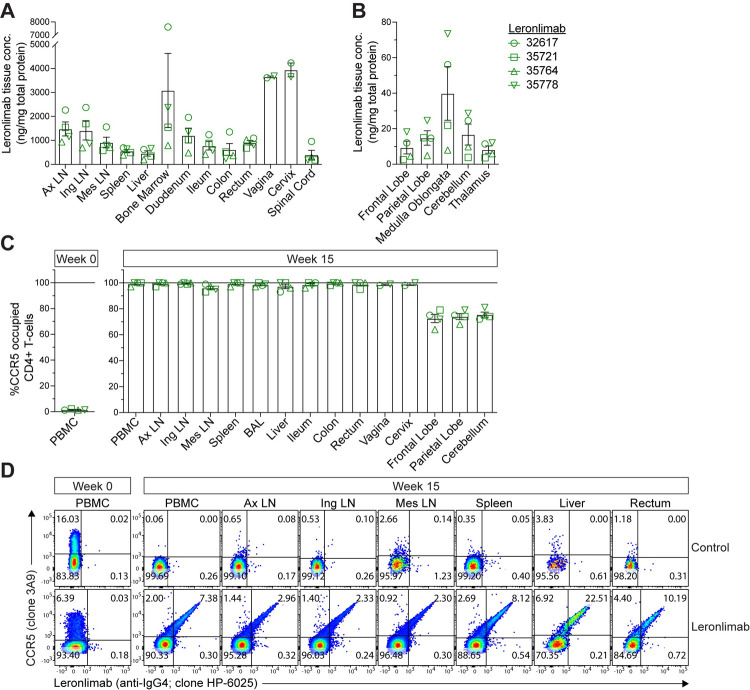
The CCR5-specific antibody Leronlimab is being investigated as a novel immunotherapy that can suppress HIV replication with minimal side effects. Here we studied the virological and immunological consequences of Leronlimab in chronically CCR5-tropic HIV-1 infected humans (n = 5) on suppressive antiretroviral therapy (ART) and in ART-naïve acutely CCR5-tropic SHIV infected rhesus macaques (n = 4). All five human participants transitioned from daily combination ART to self-administered weekly subcutaneous (SC) injections of 350 mg or 700 mg Leronlimab and to date all participants have sustained virologic suppression for over seven years. In all participants, Leronlimab fully occupied CCR5 receptors on peripheral blood CD4+ T cells and monocytes. In ART-naïve rhesus macaques acutely infected with CCR5-tropic SHIV, weekly SC injections of 50 mg/kg Leronlimab fully suppressed plasma viremia in half of the macaques. CCR5 receptor occupancy by Leronlimab occurred concomitant with rebound of CD4+ CCR5+ T-cells in peripheral blood, and full CCR5 receptor occupancy was found in multiple anatomical compartments. Our results demonstrate that weekly, self-administered Leronlimab was safe, well-tolerated, and efficacious for long-term virologic suppression and should be included in the arsenal of safe, easily administered, longer-acting antiretroviral treatments for people living with HIV-1. Trial Registration: ClinicalTrials.gov Identifiers: NCT02175680 and NCT02355184.
Conflict of interest statement
I have read the journal’s policy and the authors of this manuscript have the following competing interests: JBS and LCN have received compensation for serving on the scientific advisory board of CytoDyn, a company that may have commercial interests in the results of this research. JBS, HLW, and GMW have also received compensation for consulting for CytoDyn. The potential conflict of interest has been reviewed and managed by the Oregon Health & Science University. LCN has served as an advisor for Abbvie and ViiV Healthcare unrelated to this study. NP and SK are employees of CytoDyn, owner and developer of Leronlimab. KD is an employee of Amarex Clinical Research, a company that manages clinical trials and regulatory matters for CytoDyn. All other authors declare no competing interests. Authors Kush Dhody, Nader Pourhassan, and Cassandra Moats were unavailable to confirm their authorship contributions. On their behalf, the corresponding author has reported their contributions to the best of their knowledge.
Figures



References
-
- HIV drug resistance report 2017. Geneva: World Health Organization; 2017.
-
- Phillips AN, Stover J, Cambiano V, Nakagawa F, Jordan MR, Pillay D, et al. Impact of HIV Drug Resistance on HIV/AIDS-Associated Mortality, New Infections, and Antiretroviral Therapy Program Costs in Sub-Saharan Africa. J Infect Dis. 2017;215:1362–1365. doi: 10.1093/infdis/jix089 - DOI - PMC - PubMed
-
- Global action plan on HIV drug resistance 2017–2021. Geneva: World Health Organization. 2017.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
