

Multisite Retrospective Review of Outcomes in Renal Replacement Therapy for Neonates with Inborn Errors of Metabolism
- PMID: 35358588
- PMCID: PMC9233075
- DOI: 10.1016/j.jpeds.2022.03.043
Multisite Retrospective Review of Outcomes in Renal Replacement Therapy for Neonates with Inborn Errors of Metabolism
Abstract
Objective: To assess the outcomes of neonates in a contemporary multi-institutional cohort who receive renal replacement therapy (RRT) for hyperammonemia.
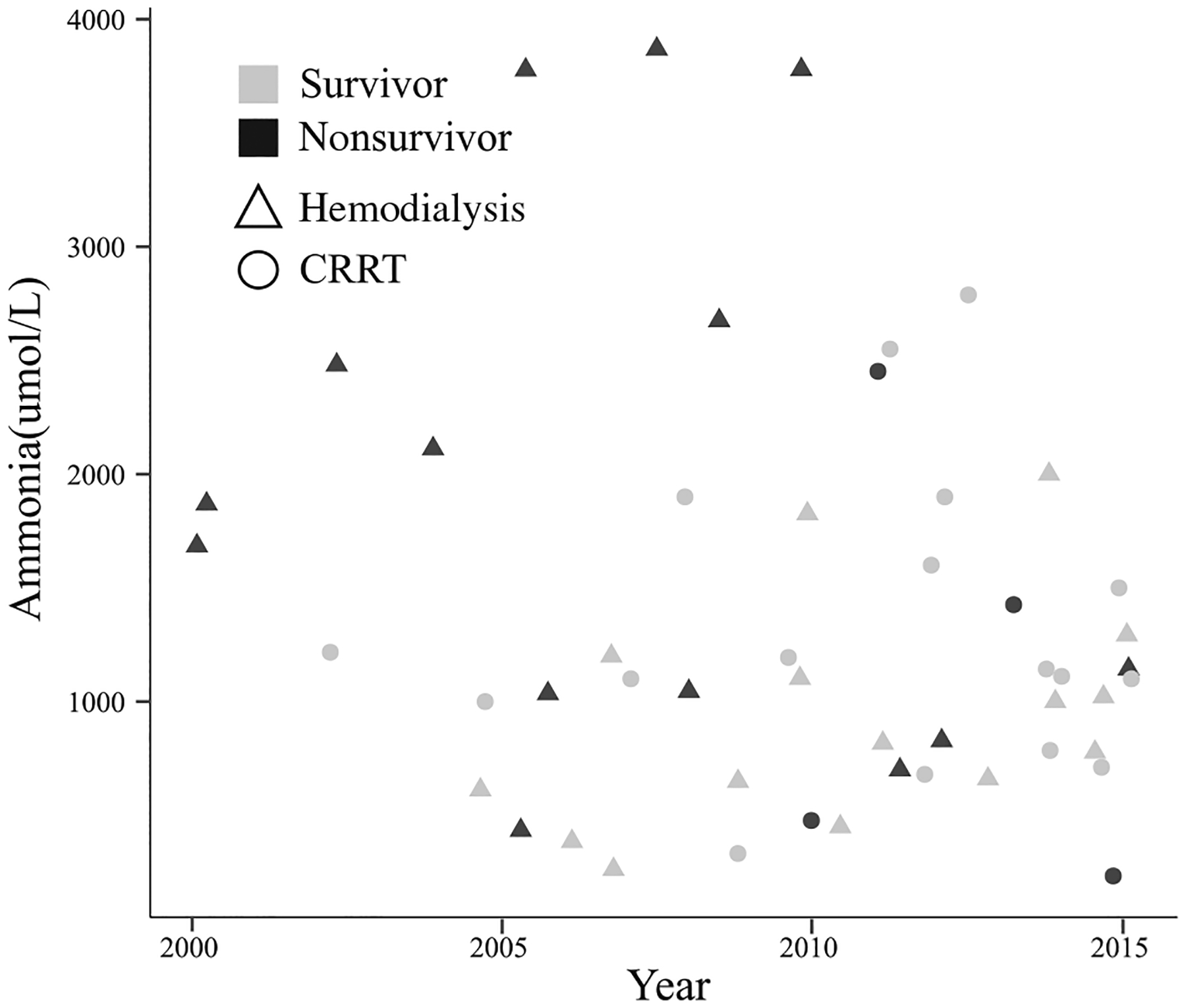
Study design: We performed a retrospective analysis of 51 neonatal patients with confirmed inborn errors of metabolism that were treated at 9 different children's hospitals in the US between 2000 and 2015.
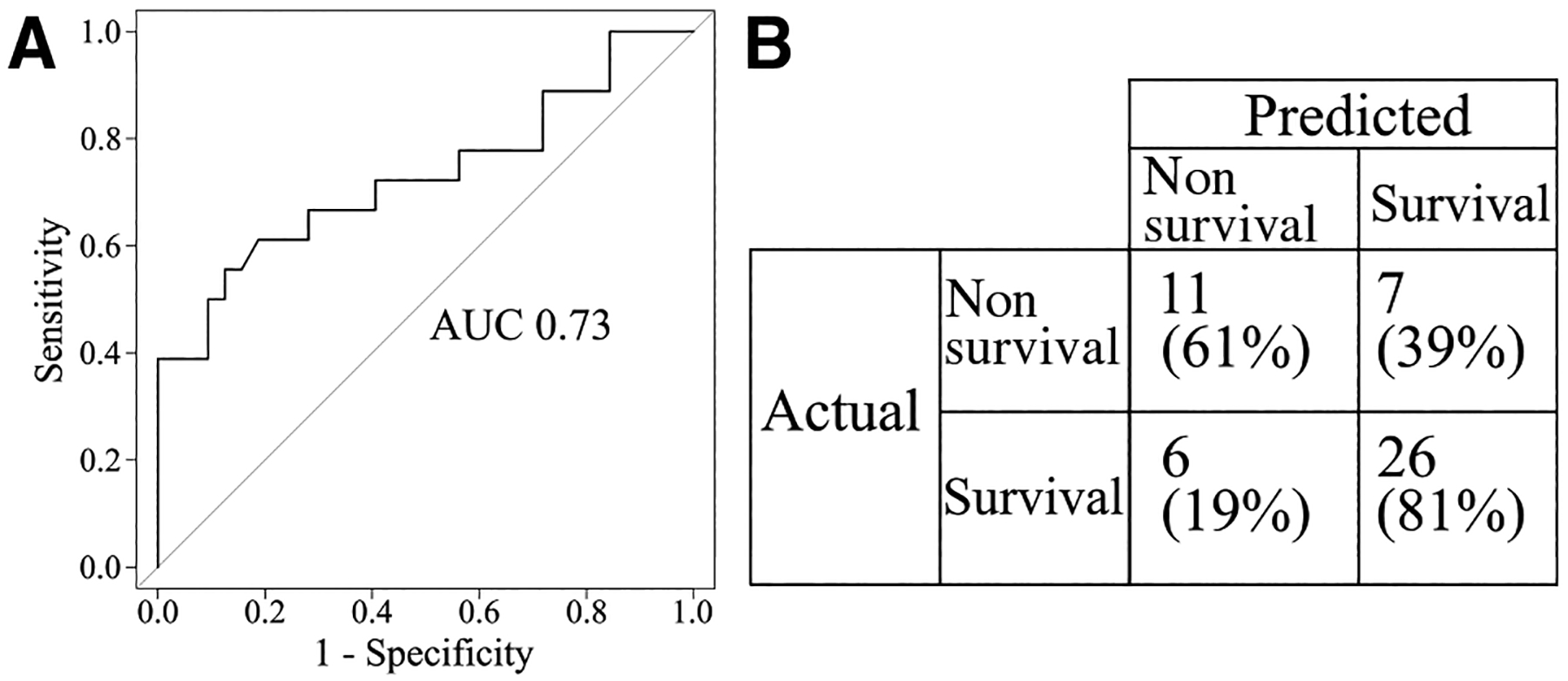
Results: Twenty-nine patients received hemodialysis (57%), 21 patients received continuous renal replacement therapy (41%), and 1 patient received peritoneal dialysis (2%). The median age at admission of both survivors (n = 33 [65%]) and nonsurvivors (n = 18) was 3 days. Peak ammonia and ammonia at admission were not significantly different between survivors and nonsurvivors. Hemodialysis, having more than 1 indication for RRT in addition to hyperammonemia, and complications during RRT were all risk factors for mortality. After accounting for multiple patient factors by multivariable analyses, hemodialysis was associated with a higher risk of death compared with continuous renal replacement therapy. When clinical factors including evidence of renal dysfunction, number of complications, concurrent extracorporeal membrane oxygenation, vasopressor requirement, and degree of hyperammonemia were held constant in a single Cox regression model, the hazard ratio for death with hemodialysis was 4.07 (95% CI 0.908-18.2, P value = .067). To help providers caring for neonates with hyperammonemia understand their patient's likelihood of survival, we created a predictive model with input variables known at the start of RRT.
Conclusions: Our large, multicenter retrospective review supports the use of continuous renal replacement therapy for neonatal hyperammonemia.
Keywords: IEM; RRT; ammonia; dialysis; survival.
Copyright © 2022 Elsevier Inc. All rights reserved.
Figures
References
-
- Burton BK. Inborn errors of metabolism in infancy: a guide to diagnosis. Pediatrics 1998;102:E69. - PubMed
-
- Auron A, Brophy PD. Hyperammonemia in review: pathophysiology, diagnosis, and treatment. Pediatr Nephrol 2012;27:207–22. - PubMed
-
- Kido J, Nakamura K, Mitsubuchi H, Ohura T, Takayanagi M, Matsuo M, et al. Long-term outcome and intervention of urea cycle disorders in Japan. J Inherit Metab Dis 2012;35:777–85. - PubMed
-
- Ames EG, Luckritz KE, Ahmad A. A retrospective review of outcomes in the treatment of hyperammonemia with renal replacement therapy due to inborn errors of metabolism. Pediatr Nephrol 2020;35:1761–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
