

A Novel Nomogram for Predicting Postoperative Liver Failure After Major Hepatectomy for Hepatocellular Carcinoma
- PMID: 35359352
- PMCID: PMC8964030
- DOI: 10.3389/fonc.2022.817895
A Novel Nomogram for Predicting Postoperative Liver Failure After Major Hepatectomy for Hepatocellular Carcinoma
Abstract
Background: Post-hepatectomy liver failure (PHLF) is the most common cause of mortality after major hepatectomy in hepatocellular carcinoma (HCC) patients. We aim to develop a nomogram to preoperatively predict grade B/C PHLF defined by the International Study Group on Liver Surgery Grading (ISGLS) in HCC patients undergoing major hepatectomy.
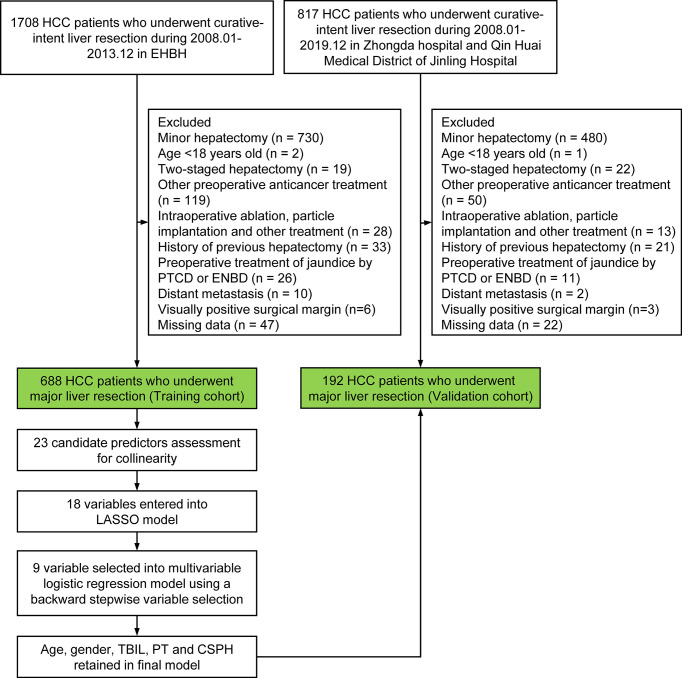
Study design: The consecutive HCC patients who underwent major hepatectomy at the Eastern Hepatobiliary Surgery Hospital between 2008 and 2013 served as a training cohort to develop a preoperative nomogram, and patients from 2 other hospitals comprised an external validation cohort. Least absolute shrinkage and selection operator (LASSO) logistic regression was applied to identify preoperative predictors of grade B/C PHLF. Multivariable logistic regression was utilized to establish a nomogram model. Internal and external validations were used to verify the performance of the nomogram. The accuracy of the nomogram was also compared with the conventional scoring models, including MELD and ALBI score.
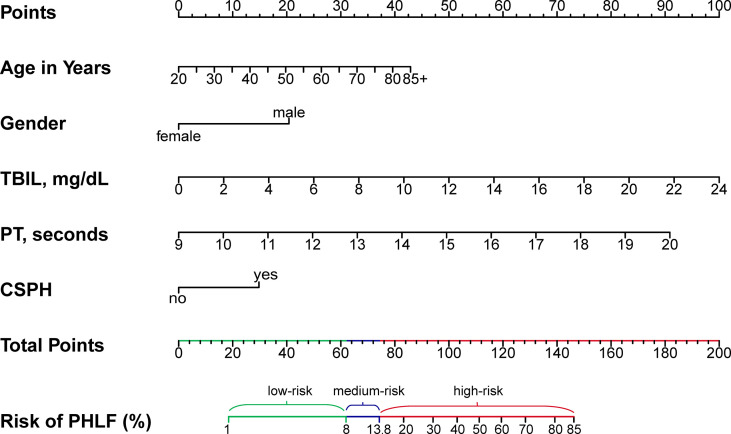
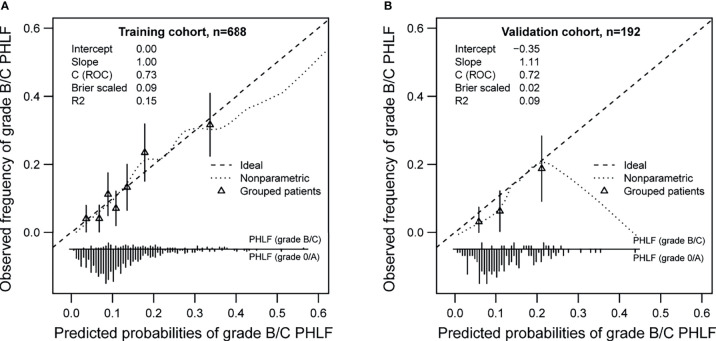
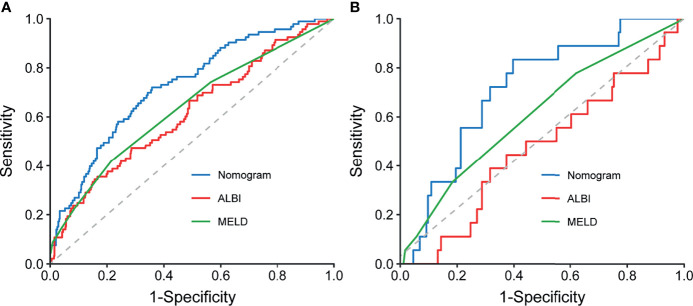
Results: A total of 880 patients who underwent major hepatectomy (668 in the training cohort and 192 in the validation cohort) were enrolled in this study. The independent risk factors of grade B/C PHLF were age, gender, prothrombin time, total bilirubin, and CSPH, which were incorporated into the nomogram. Good prediction discrimination was achieved in the training (AUROC: 0.73) and validation (AUROC: 0.72) cohorts. The calibration curve also showed good agreement in both training and validation cohorts. The nomogram has a better performance than MELD and ALBI score models.
Conclusion: The proposed nomogram showed more accurate ability to individually predict grade B/C PHLF after major hepatectomy in HCC patients than MELD and ALBI scores.
Keywords: hepatocellular carcinoma; major hepatectomy; nomogram; post-hepatectomy liver failure; prediction model.
Copyright © 2022 Lei, Cheng, Si, Yang, Guo, Ma, Yu, Wang and Cheng.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Shi J-Y, Sun L-Y, Quan B, Xing H, Li C, Liang L, et al. A Novel Online Calculator Based on Noninvasive Markers (ALBI and APRI) for Predicting Post-Hepatectomy Liver Failure in Patients With Hepatocellular Carcinoma. Clin Res Hepatol Gastroenterol (2021) 45(4):101534. doi: 10.1016/j.clinre.2020.09.001 - DOI - PubMed
LinkOut - more resources
Full Text Sources