

Trends in Disease Burden of Chronic Lymphocytic Leukemia at the Global, Regional, and National Levels From 1990 to 2019, and Projections Until 2030: A Population-Based Epidemiologic Study
- PMID: 35359356
- PMCID: PMC8961301
- DOI: 10.3389/fonc.2022.840616
Trends in Disease Burden of Chronic Lymphocytic Leukemia at the Global, Regional, and National Levels From 1990 to 2019, and Projections Until 2030: A Population-Based Epidemiologic Study
Abstract
Background: The prognosis of chronic lymphocytic leukemia (CLL) has been improved dramatically, but there are limited studies focusing on CLL disease burden on a global scale. We aimed to evaluate the accurate assessment of the disease burden of CLL that may provide more detailed epidemiological information for rational policies.
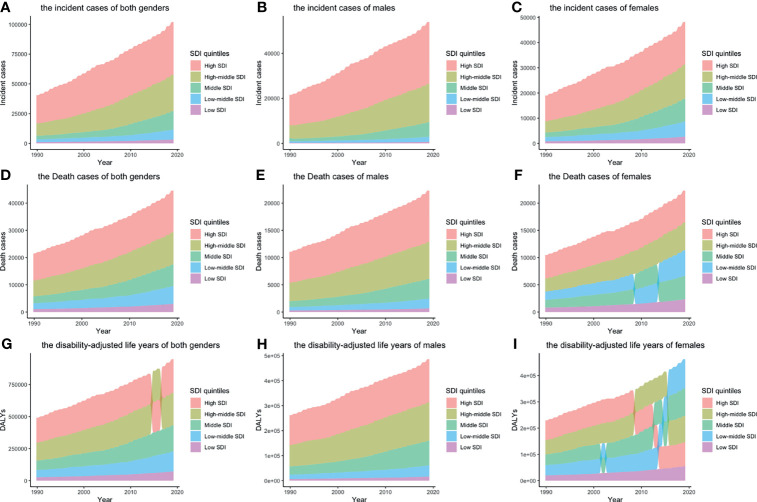
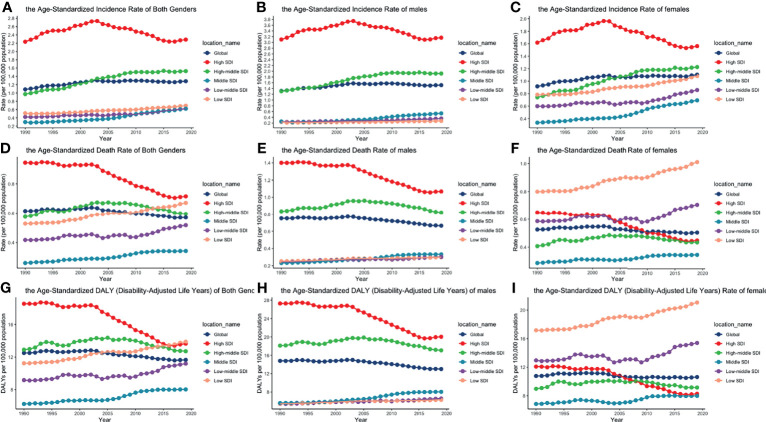
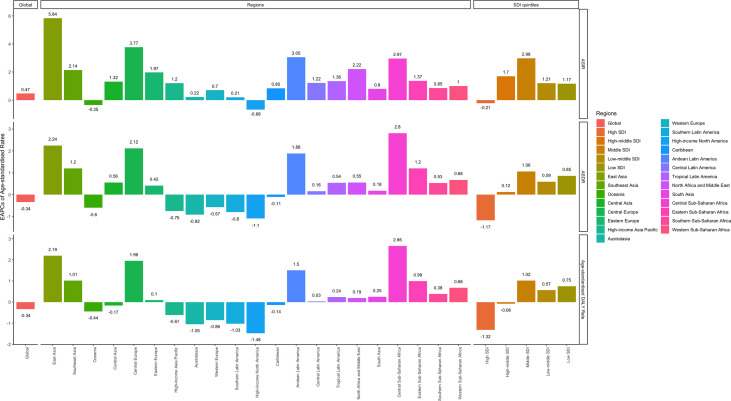
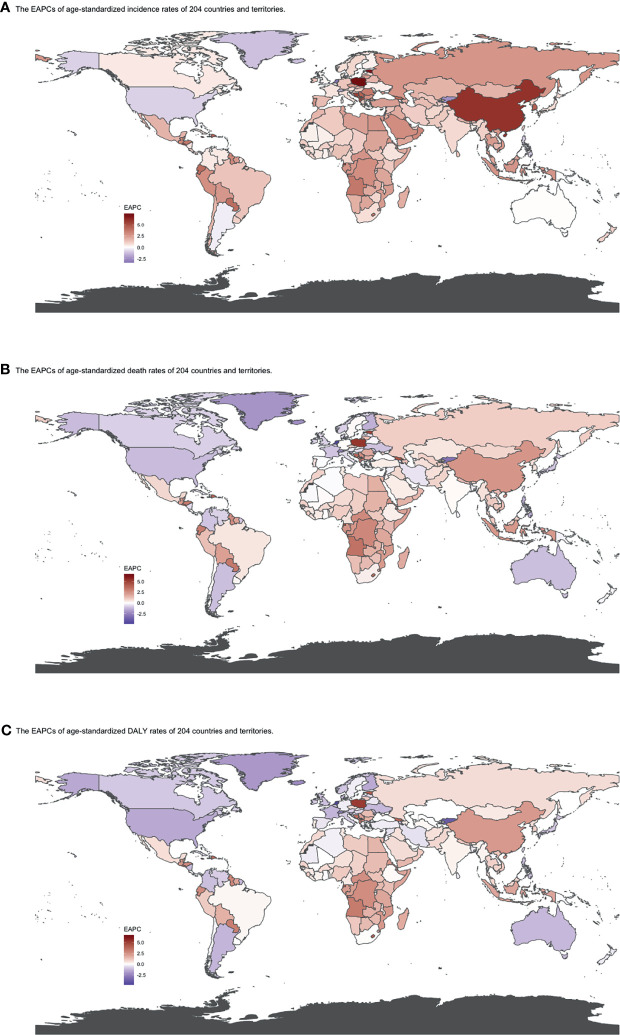
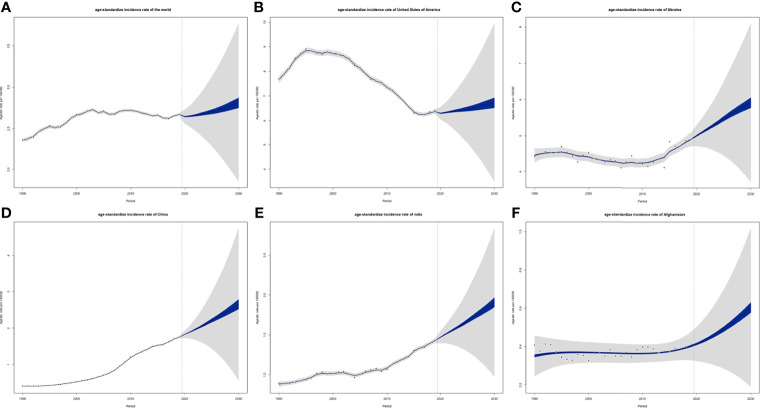
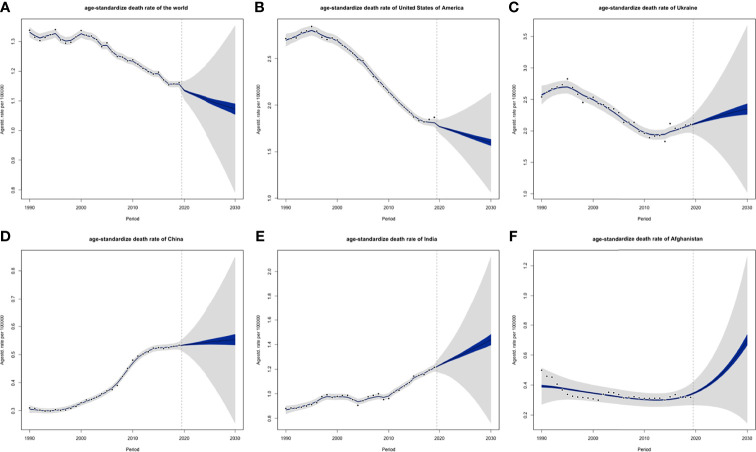
Methods: The main source of the data was the Global Burden of Disease (GBD) study 2019. Incident cases, death cases, disability-adjusted life years (DALYs), and their corresponding age-standardized rates (ASRs) from 1990 to 2019 were used to describe the burden of CLL. Data about attributable risk factors were also extracted and analyzed. Bayesian age-period-cohort (BAPC) models were used to assess and project the incidence and mortality rates till 2030.
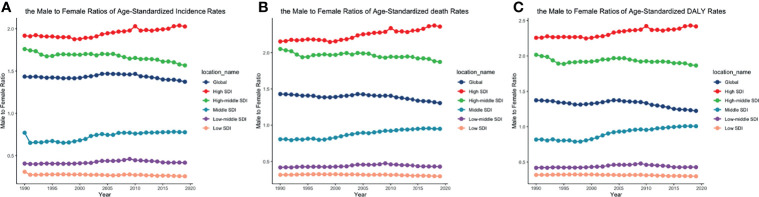
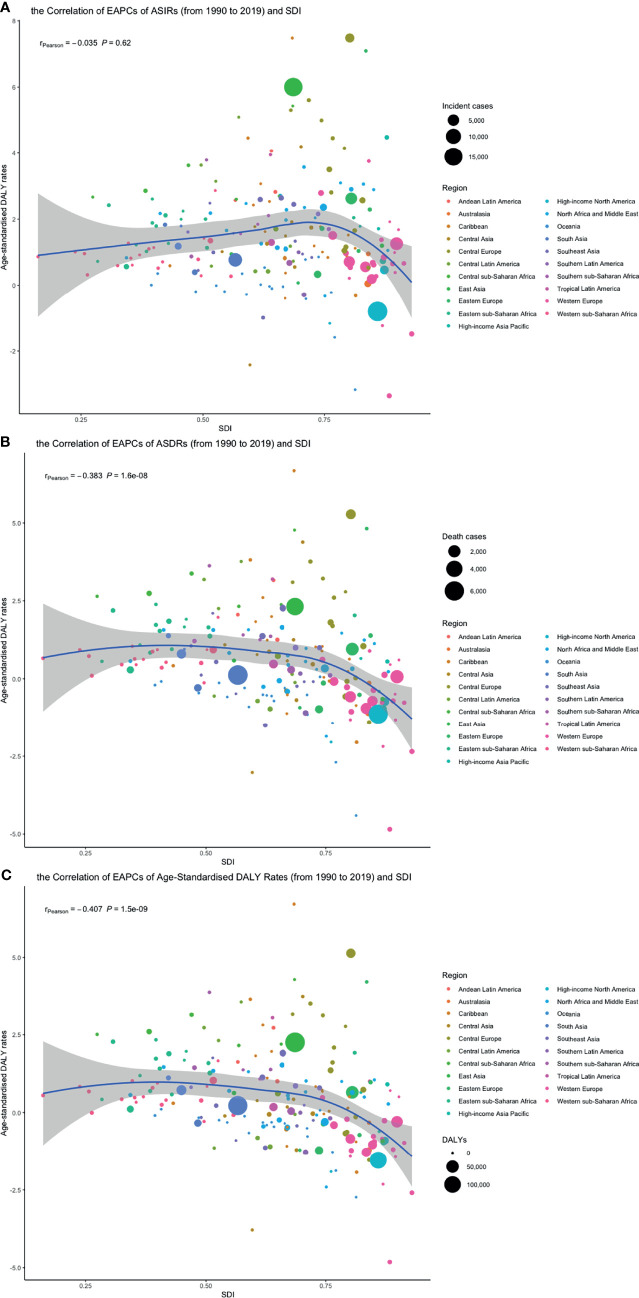
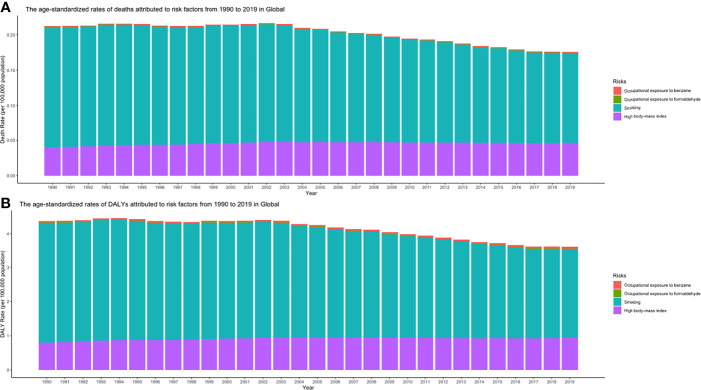
Results: Globally, the incidence of CLL had been increasing. Deaths and DALYs decreased slightly. The burden of death and DALY is affected by socio-demographic index (SDI). The incidence rate, death rate, and DALY rate of CLL increased significantly with age. Male-to-female ratios of incidence rates varied in different SDI quintiles. Smoking, high body mass index, and occupational exposure to benzene or formaldehyde were the potential risk factors related to CLL. Global ASIRs might tend to increase until 2030, while ASDR would decrease until 2030.
Conclusion: The disease burden of CLL decreased in higher SDI countries but increased in lower ones. Strategies for early detection of asymptomatic CLL, development of novel drugs, and measures against attributable factors should be implemented to combat CLL burden.
Keywords: chronic lymphocytic leukemia; death; disability-adjusted life years; epidemiology; incidence.
Copyright © 2022 Ou, Long, Ji, Zhan, Qiao, Wang, Chen and Cheng.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures





References
LinkOut - more resources
Full Text Sources