

doi: 10.4103/aian.AIAN_744_20.
Epub 2021 May 21.
Recurrent Posterior Circulation Stroke as An Initial Manifestation of Atlantoaxial Dislocation in a Child
Affiliations
- PMID: 35359524
- PMCID: PMC8965939
- DOI: 10.4103/aian.AIAN_744_20
Item in Clipboard
Recurrent Posterior Circulation Stroke as An Initial Manifestation of Atlantoaxial Dislocation in a Child
Ann Indian Acad Neurol.
2021 Nov-Dec.
No abstract available
Conflict of interest statement
There are no conflicts of interest.
Figures
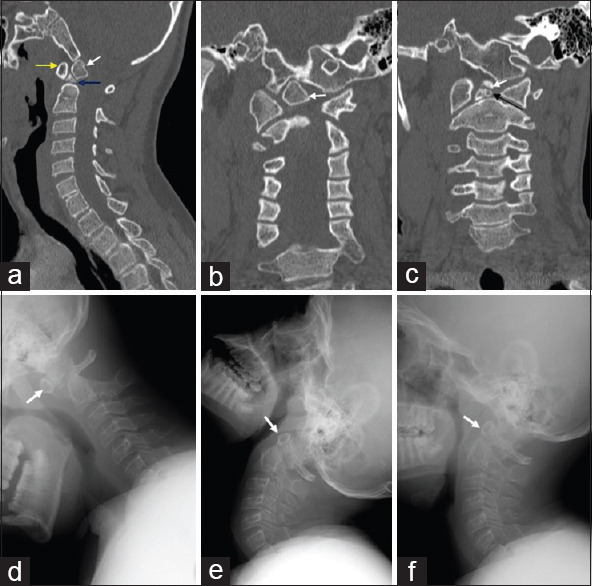
Sagittal reformat (a) of noncontrast cervical CT shows a cleft in the basal odontoid (blue arrow) suggestive of a midline integration defect with persistent ossiculum terminale (white arrow). Note hypertrophied anterior arch of atlas (yellow arrow). Coronal reformat (b, c) of the same shows persistent ossiculum terminale (white arrow in b and c) with midline integration defect of the basal odontoid (black arrow in b). Lateral cervical radiograph in flexion (d) shows anterior displacement of the anterior arch of atlas and ossiculum terminale (arrow) relative to the position in extension (arrow in e) and neutral position (arrow in f)

Sagittal T2 weighted image (a) shows persistent ossiculum terminale (white arrowhead) with midline integration defect of the basal odontoid (yellow arrow). Loss of flow void is seen in the basilar artery (red arrow) with a chronic infarct in the pons (black arrow). Axial T2 weighted images (b, c) show a chronic pontine infarct (black arrow in b) with loss of flow void in V4 segment of both vertebral arteries (arrowheads in c). TOF-MRA (d, e) show nonvisualization of both vertebral arteries and the basilar artery with bilateral fetal posterior cerebral arteries (arrows in d). Post-contrast axial T1-SPACE (f) shows subtle eccentric hyperintensity along the V4 segment of both vertebral arteries (white arrowheads)
Similar articles
-
Pediatric posterior cerebral artery stroke as a presentation of atlantoaxial dislocation.J Pediatr Neurosci. 2015 Apr-Jun;10(2):149-52. doi: 10.4103/1817-1745.159186. J Pediatr Neurosci. 2015. PMID: 26167221 Free PMC article.
-
Posterior Screw-Rod Fixation and Selective Axial Loosening for the Treatment of Atlantoaxial Instability or Dislocation Caused by Os Odontoideum: A Case Series for a Single Posterior Approach.World Neurosurg. 2019 Dec;132:e193-e201. doi: 10.1016/j.wneu.2019.08.208. Epub 2019 Sep 4. World Neurosurg. 2019. PMID: 31493594
-
[The synthetic typing and its clinical application in atlantoaxial dislocation].Zhonghua Wai Ke Za Zhi. 2008 Feb 15;46(4):280-2. Zhonghua Wai Ke Za Zhi. 2008. PMID: 18683765 Chinese.
-
Posterior atlantoaxial dislocation without fracture or neurological symptoms treated by transoral-posterior approach surgery: a case report and literature review.Eur Spine J. 2019 Jun;28(Suppl 2):37-40. doi: 10.1007/s00586-018-5823-6. Epub 2018 Nov 17. Eur Spine J. 2019. PMID: 30448988 Review.
-
Management of Unusual Atlantoaxial Dislocation.Spine (Phila Pa 1976). 2017 Apr 15;42(8):573-577. doi: 10.1097/BRS.0000000000001872. Spine (Phila Pa 1976). 2017. PMID: 28399555 Review.
References
-
- Mallick AA, Ganesan V, Kirkham FJ, Fallon P, Hedderly T, McShane T, et al. Childhood arterial ischaemic stroke incidence, presenting features, and risk factors: A prospective population-based study. Lancet Neurol. 2014;13:35–43. - PubMed
-
- Bharucha EP, Dastur HM. Craniovertebral Anomalies (A Report on 40 Cases) Brain J Neurol. 1964;87:469–80. - PubMed
-
- Ganesan V, Chong WK, Cox TC, Chawda SJ, Prengler M, Kirkham FJ. Posterior circulation stroke in childhood: Risk factors and recurrence. Neurology. 2002;59:1552–6. - PubMed
-
- Shim SC, Yoo DH, Lee JK, Koh HK, Lee SR, Oh SH, et al. Multiple cerebellar infarction due to vertebral artery obstruction and bulbar symptoms associated with vertical subluxation and atlanto-occipital subluxation in ankylosing spondylitis. J Rheumatol. 1998;25:2464–8. - PubMed
