

Efficacy and Safety of Daprodustat Vs rhEPO for Anemia in Patients With Chronic Kidney Disease: A Meta-Analysis and Trial Sequential Analysis
- PMID: 35359863
- PMCID: PMC8961323
- DOI: 10.3389/fphar.2022.746265
Efficacy and Safety of Daprodustat Vs rhEPO for Anemia in Patients With Chronic Kidney Disease: A Meta-Analysis and Trial Sequential Analysis
Abstract
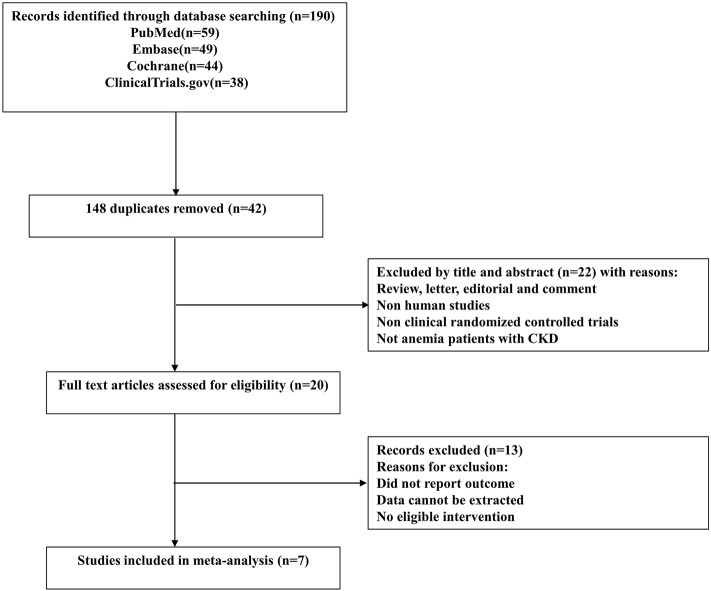
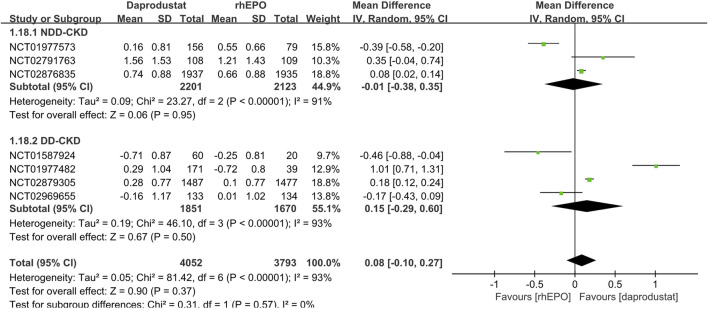
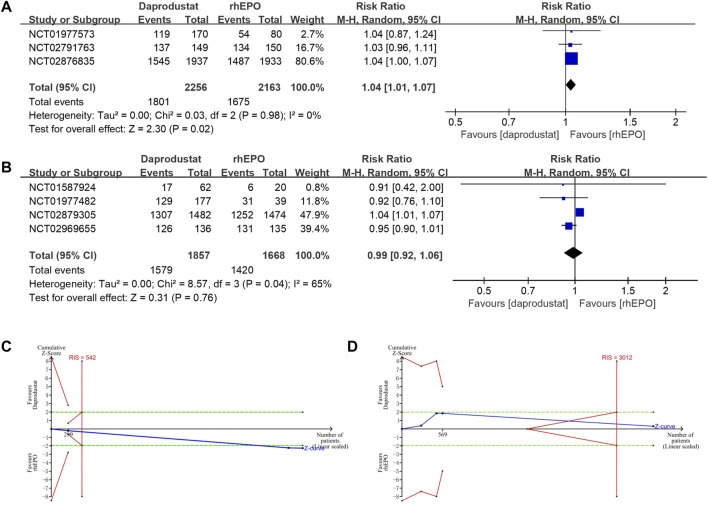
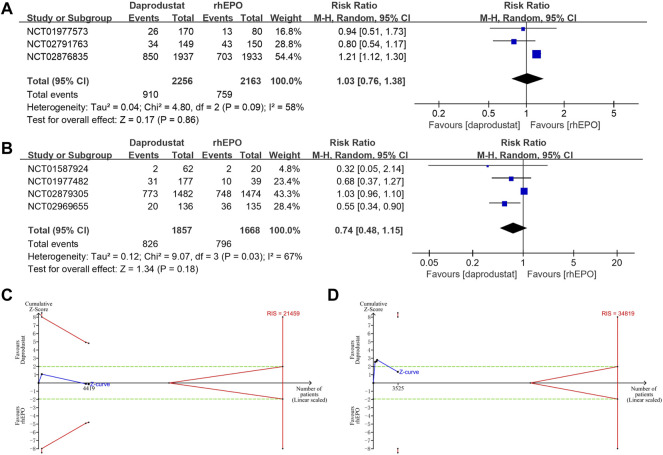
Introduction: Daprodustat, a novel hypoxia-inducible factor prolyl-hydroxylase inhibitor (HIF-PHI), its efficacy and safety remain unclear. Thus, we conducted this meta-analysis aiming at investigating its efficacy and safety on the treatment of patients with chronic kidney disease (CKD)-related anemia. Methods: We systematically searched for relevant studies in PubMed, Embase, Cochrane Library and Clinical Trial Registries databases from inception until December 2021. We selected randomized controlled trials comparing daprodustat with recombinant human erythropoietin (rhEPO) in anemia patients with CKD with or without dialysis. Results: Seven studies including 7933 patients met the inclusion criteria. For both nondialysis-dependent (NDD-) CKD and dialysis-dependent (DD-) CKD patients, the pooled results showed that there was no significant difference in the changes in hemoglobin levels between the daprodustat and rhEPO groups (mean difference (MD) = -0.01, 95% confidence interval (CI) = -0.38, 0.35, p = 0.95; MD = 0.15, 95% CI = -0.29, 0.60, p = 0.50; respectively). In addition, a significant increase in transferrin saturation (TSAT), total iron binding capacity (TIBC) and total iron was observed in daprodustat groups compared with rhEPO groups in DD-CKD patients (p < 0.05). As for safety, the overall frequency of adverse events was similar between the daprodustat and rhEPO groups in DD-CKD patients (relative risk (RR) = 0.99, 95%CI = 0.92, 1.06, p = 0.76), and the trial sequential analysis (TSA) confirmed this result. But for NDD-CKD patients, the incidence of adverse events in the daprodustat groups was significantly higher than that of rhEPO groups (RR = 1.04, 95%CI = 1.01,1.07, p = 0.02), while the TSA corrected this result. No trend of increasing incidence of serious adverse events was found in all daprodustat treated patients, but the TSA could not confirm this result. Conclusion: Although daprodustat was noninferior to rhEPO in correcting anemia in both NDD-CKD and DD-CKD patients, it seemed to have a better effect on optimizing iron metabolism in DD-CKD patients. Daprodustat may be a promising alternative for the treatment of anemia in patients with CKD. However, due to the lack of included studies, future researches are needed to further evaluate the therapeutic effect of daprodustat. Systematic Review Registration: https://www.crd.york.ac.uk/prospero/, identifier CRD42021229636.
Keywords: anemia; chronic kidney disease; daprodustat; meta-analysis; trial sequential analysis.
Copyright © 2022 Fu, Geng, Chi, Song, Wu, Liu and Hong.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Efficacy and Safety of Daprodustat for Anemia Therapy in Chronic Kidney Disease Patients: A Systematic Review and Meta-Analysis.Front Pharmacol. 2021 Jan 12;11:573645. doi: 10.3389/fphar.2020.573645. eCollection 2020. Front Pharmacol. 2021. PMID: 33597868 Free PMC article.
-
Evaluating the safety and efficacy of daprodustat for anemia of chronic kidney disease: a meta-analysis of randomized clinical trials.Eur J Clin Pharmacol. 2022 Dec;78(12):1867-1875. doi: 10.1007/s00228-022-03395-y. Epub 2022 Oct 5. Eur J Clin Pharmacol. 2022. PMID: 36195739 Review.
-
Safety and Efficacy of Roxadustat for Anemia in Patients With Chronic Kidney Disease: A Meta-Analysis and Trial Sequential Analysis.Front Med (Lausanne). 2021 Aug 31;8:724456. doi: 10.3389/fmed.2021.724456. eCollection 2021. Front Med (Lausanne). 2021. PMID: 34532333 Free PMC article.
-
Daprodustat for anemia: a 24-week, open-label, randomized controlled trial in participants with chronic kidney disease.Clin Kidney J. 2019 Feb;12(1):129-138. doi: 10.1093/ckj/sfy013. Epub 2018 Mar 9. Clin Kidney J. 2019. PMID: 30746140 Free PMC article.
-
Safety and Efficacy of Hypoxia-Inducible Factor-Prolyl Hydroxylase Inhibitors vs. Erythropoietin-Stimulating Agents in Treating Anemia in Renal Patients (With or Without Dialysis): A Meta-Analysis and Systematic Review.Cureus. 2023 Oct 21;15(10):e47430. doi: 10.7759/cureus.47430. eCollection 2023 Oct. Cureus. 2023. PMID: 38021836 Free PMC article. Review.
Cited by
-
Impact of C-reactive protein on the effect of Roxadustat for the treatment of anemia in chronic kidney disease: a systematic review of randomized controlled trials.BMC Nephrol. 2024 Feb 5;25(1):47. doi: 10.1186/s12882-024-03474-5. BMC Nephrol. 2024. PMID: 38311719 Free PMC article.
-
Comparison of outcomes on hypoxia-inducible factor prolyl hydroxylase inhibitors (HIF-PHIs) in anaemia associated with chronic kidney disease: network meta-analyses in dialysis and non-dialysis dependent populations.Clin Kidney J. 2023 Dec 7;17(1):sfad298. doi: 10.1093/ckj/sfad298. eCollection 2024 Jan. Clin Kidney J. 2023. PMID: 38250252 Free PMC article.
-
Daprodustat.Hosp Pharm. 2023 Dec;58(6):530-543. doi: 10.1177/00185787231172382. Epub 2023 May 17. Hosp Pharm. 2023. PMID: 38560540 Free PMC article. Review.
-
The Efficacy and Safety of Roxadustat for Anemia in Hemodialysis Patients with Chronic Kidney Disease: A Meta-Analysis of Randomized Controlled Trials.Toxics. 2024 Nov 25;12(12):846. doi: 10.3390/toxics12120846. Toxics. 2024. PMID: 39771061 Free PMC article.
-
Risk factors and outcomes of intraoperative blood transfusion in elderly patients undergoing gastrointestinal cancer surgery.World J Gastrointest Surg. 2025 Jul 27;17(7):105860. doi: 10.4240/wjgs.v17.i7.105860. World J Gastrointest Surg. 2025. PMID: 40740924 Free PMC article.
References
-
- Akizawa T., Nangaku M., Yonekawa T., Okuda N., Kawamatsu S., Onoue T., et al. (2020). Efficacy and Safety of Daprodustat Compared with Darbepoetin Alfa in Japanese Hemodialysis Patients with Anemia: A Randomized, Double-Blind, Phase 3 Trial. Clin. J. Am. Soc. Nephrol. 15 (8), 1155–1165. 10.2215/CJN.16011219 - DOI - PMC - PubMed
-
- Asikainen T. M., Ahmad A., Schneider B. K., Ho W. B., Arend M., Brenner M., et al. (2005). Stimulation of HIF-1alpha, HIF-2alpha, and VEGF by Prolyl 4-hydroxylase Inhibition in Human Lung Endothelial and Epithelial Cells. Free Radic. Biol. Med. 38 (8), 1002–1013. 10.1016/j.freeradbiomed.2004.12.004 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous